Joint Pathology Center
Veterinary Pathology Services
Wednesday Slide Conference
2018-2019
Conference 11
5 December, 2018
CASE IV: E2337 (JPC 4090973)
Signalment: 8-year-old castrated male domestic shorthair cat, Felis catus
History: Presented with a 1cm mass around the right lower canine. The referring veterinarian removed the mass, tooth, and part of the mandible.
Gross Pathology: None given.
Laboratory results: None given.
Microscopic Description:
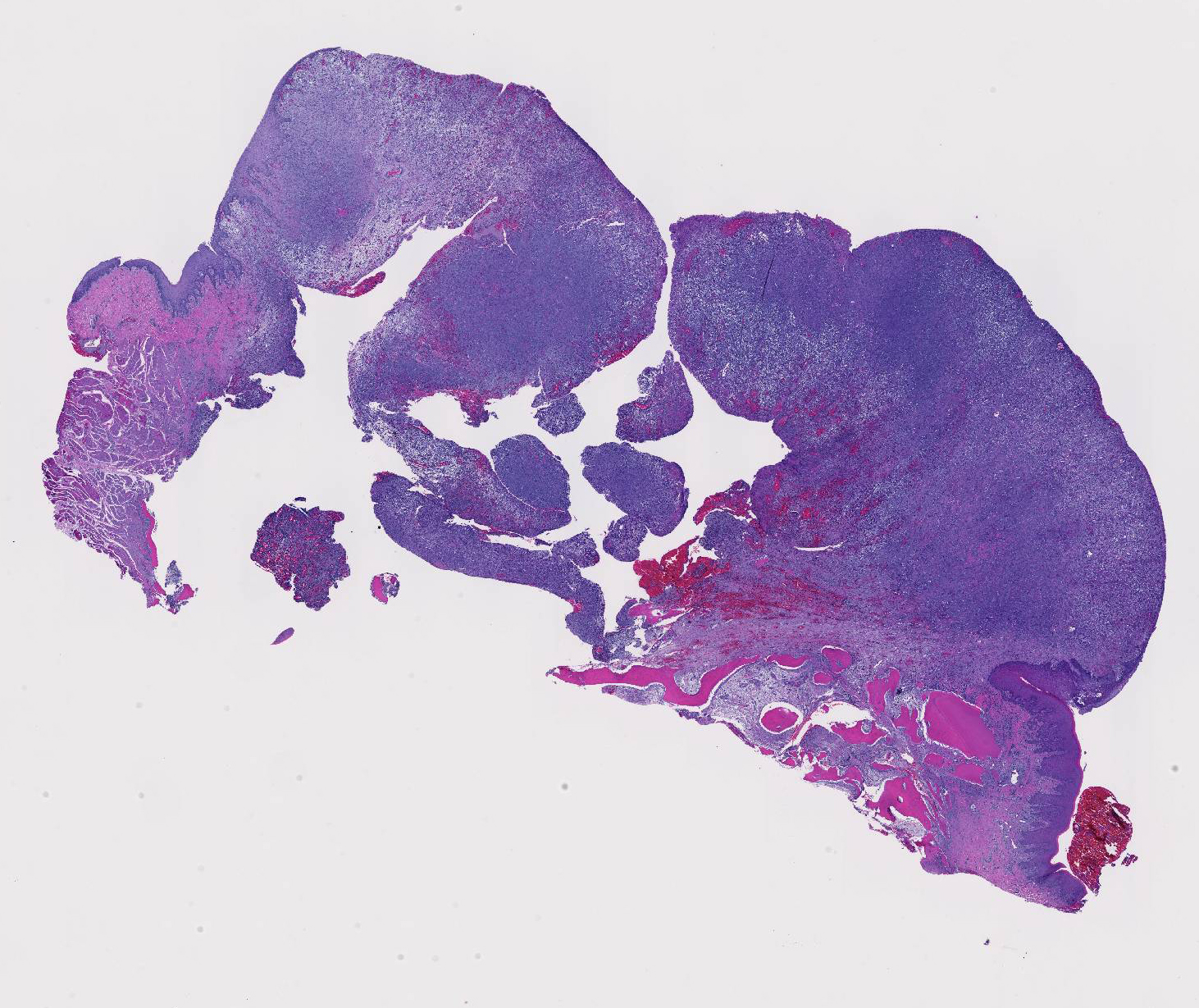
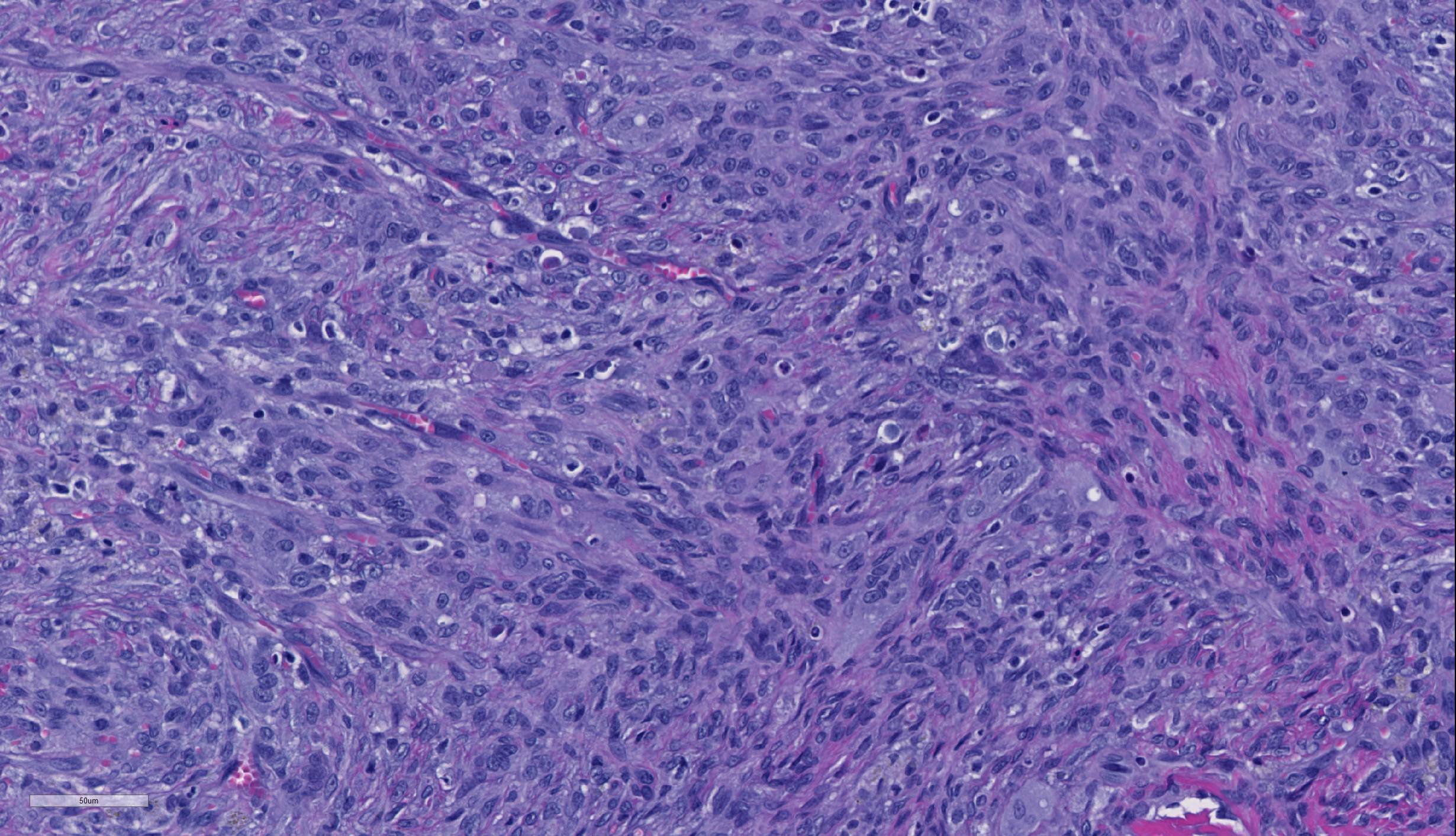
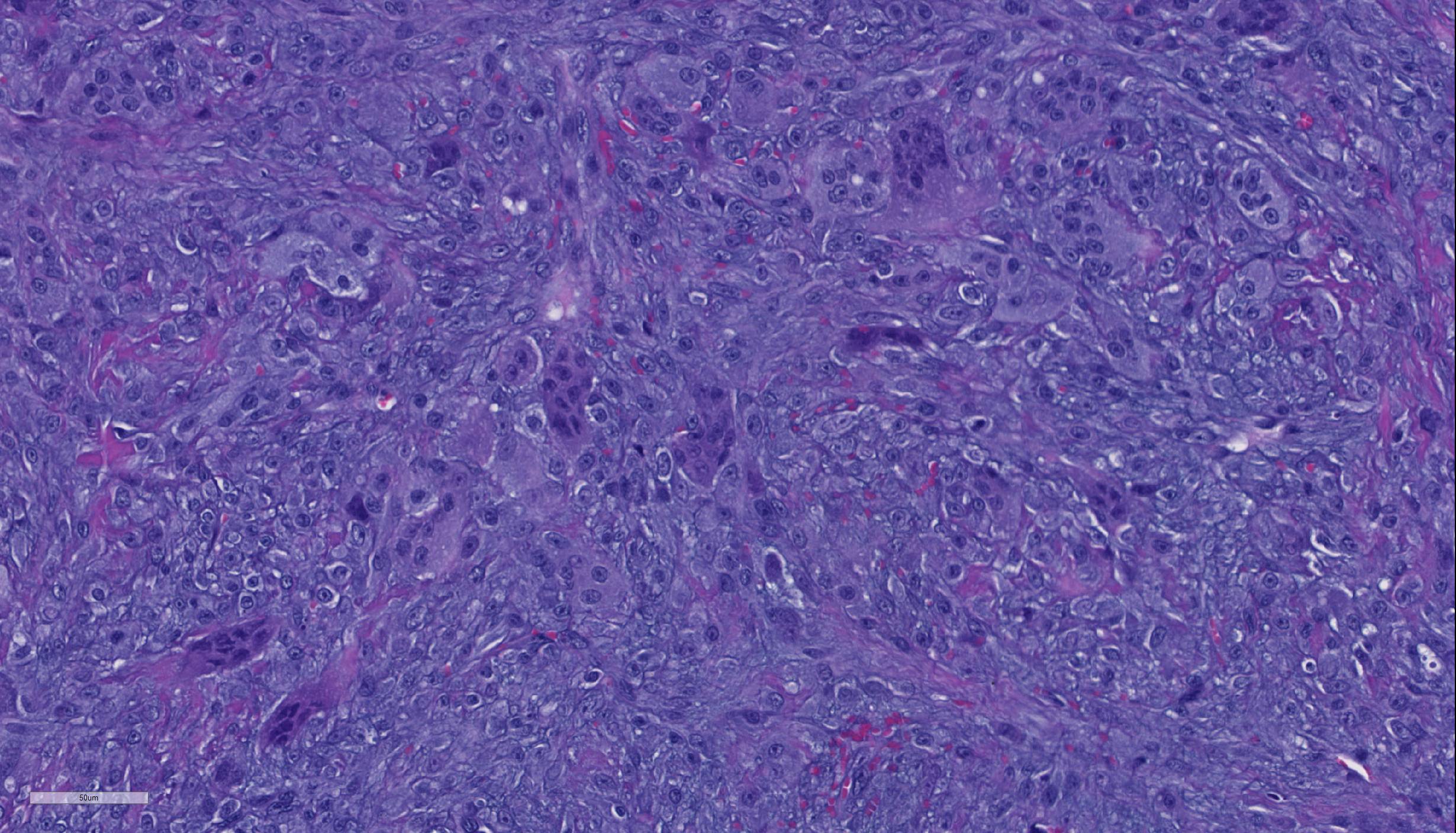
There is almost diffuse gingival ulceration with necrosis of the exposed lamina propria, fibrin deposition, and neutrophil infiltration. Underlying this there is early granulation tissue proliferation that blends into a deeper, poorly-demarcated population of plump spindle cells arranged in streams and admixed with large numbers of multinucleated giant cells. Cells are occasionally separated by amorphous eosinophilic material (presumed osteoid). The nuclei have finely stippled chromatin and a central prominent nucleolus. This area is surrounded by fibrosis with scattered lymphocytes and plasma cells. Occasionally there are central areas of necrosis with hemorrhage, neutrophils, and rarely a raft of filamentous bacteria is present (in some slides). At the periphery of the mass there are fragments of pre-existing lamellar bone with varying amounts of woven bone. Bone fragments are lined by primarily by osteoblasts with rare osteoclasts in Howship’s lacunae. There are also tooth fragments surrounded by fibrosis. The remaining gingival epithelium is hyperplastic.
Contributor’s Morphologic Diagnoses:
Gingiva: Peripheral giant cell granuloma
Contributor’s Comment: Peripheral giant cell granulomas were previously referred to as giant cell epulides.7 These are ulcerated masses composed of a poorly demarcated proliferation of fibroblasts and blood vessels (resembling granulation tissue) with prominent multinucleated giant cells. Osteoid-like material may be present. Cellular pleomorphism, mitoses and anaplastic cells are absent. Unlike the fibromatous epulis and acanthomatous ameloblastoma, these tumors lack an epithelial component, although the gingival epithelium adjacent to the areas of ulceration is, as expected, hyperplastic.1
In cats, peripheral giant cell granulomas (giant cell epulis) are the second most common gingival tumor (28.8%) after fibromatous epulis (57.7%).The reported range for age of onset is 4-19 years. Compared to the fibromatous epulis, giant cell epulides are more likely to be ulcerated, grow more rapidly, rapidly recur following excision, and are more likely to result in the death or euthanasia of the cat.1
Immunohistochemical stains have shown the multinucleated giant cells to be positive for vimentin, tartrate-resistant acid phosphatase (TRAP; osteoclast marker) and the polyclonal antibody receptor activator of nuclear factor κβ (RANK; involved in osteoclast maturation)3 while being negative for smooth muscle actin, MIB-1 (proliferation marker) and factor VIII. These findings suggest an osteoclastic, as opposed to macrophage, origin for the multinucleated giant cells.1
Peripheral giant cell granulomas are regarded as hyperplastic (reactive) and have occurred at sites of tooth extraction.7
Contributing Institution:
University of Tennessee, College of Veterinary Medicine, Department of Biomedical and Diagnostic Sciences http://www.vet.utk.edu/departments/path/index.php
JPC Diagnosis: Gingiva: Peripheral giant cell granuloma.
JPC Comment:
The contributor does an excellent job of describing this poorly-named reactive lesion. The term “peripheral giant cell granuloma” has been lifted from the human literature, although this lesion bears no resemblance to a true granuloma. The term “peripheral” is used to differentiate this lesion from its identical intraosseous or “central” counterpart. It has been classified previously as an epulis3, another relatively non-specific term for a “tumor-like mass on the gingiva” which also appears to be falling from common usage today.
In the human, where this lesion is best defined, it represents an exuberant reparative response to local trauma or irritation. These lesions are seen exclusively in the gingiva and presumably arises from the periodontal ligament or periosteum. They typically present as red-blue, broad-based masses in the gingiva around the incisors and premolars (a location that is shared in the cat and dog as well).5 They are seen at any age in the human and tends to be seen more commonly in females than in males. . The appearance of multinucleated giant cells is unusual and the reason for the presence of this cell type remains unknown; they appear to be nonfunctional in the usual sets of either phagocytosis or bone resorption. Islands of metaplastic bone may occasionally be seen in this lesion.
A number of peripheral giant cell granulomas have been published in the dog as well.2,4 An article by DeSoutter et al.4 demonstrates an almost identical lesion in the area of the incisors or premolars (the characteristic lesion in humans as well) described as an “classic” peripheral giant cell granuloma, as well as a number of open “collision” peripheral giant cell granulomas, with features of both a peripheral giant cell granuloma and a fibromatous epulis of periodontal ligament origin. In contrast to the lesion in cats, peripheral giant cell granulomas in the dog behave more like fibromatous epulides of periodontal ligament origin and seldom recur after excision. Multinucleated cells in the canine lesion also exhibits positive staining with tartrate-resistant acid phosphatase (TRAP).
The ultimate diagnosis of this case engendered spirited discussion. A number of attendees identified osteoid amidst the spindle cell population, favoring a diagnosis of osteosarcoma in this case. Consultation from the oral pathology human subspecialists confirmed the lesion to a peripheral giant cell granuloma; the presence of osteoid is not uncommon in their experience. The presence of large islands of dental and woven bone in one area of the section, was attributed to products of the extracted tooth and section of manible surrounding it.
References:
- DeBruijn ND, Kirpensteijn J, Neyens IJS, et al. A clinicopathological study of 52 feline epulides. Vet Pathol. 2007;44:161-169.
- DeSoutter AV, Goldschmidt MH, Sanchez MD. Clinical and histologic features of 26 canine peripheral giant cell granulomas (formerly giant cell epulis). Vet Pathol 2012; 49(6): 1018-1023.
- Dubielzig RR. Tumors of Odontogenic Origin. In Head KW, Cullen JM, Dubielzig RR,Else RW, Misdorp W, Patnaik AK, Tateyama S, van der Gaag I., Histological Classification of Tumors of the Alimentary System of Domestic Animals; Second Series, Volume X. ARP Press, Bethesda, MD 2002: pp 56-57.
- Hiscox LA, Dumais Y. Peripheral Giant Cell Granuloma in a Dog. J Vet Dent; 2015 32(2): 103-110.
- Munday JS, Lohr CV, Kiupel MK. Tumors of the Alimentary Tract. In: Meuten DJ ed, Tomorsin Domestic Animals, 5th Wiley-Blackwell, Ames IA, 2017; pp: 542-543.
- Regezi JA, Sciubba JJ, Jordan RCK. Red-blue lesions. In Oral Pathology: Clinical Pathologic Correlations, 7th Elsevier Press, St. Louis MO 2017; 119-121
- Uzal FA, Plattner BL, Hostetter JM. Alimentary system. In: Jubb, Kennedy and Palmer’s Pathology of Domestic Animals.6th Elsevier 2016: vol.2 p.21.