Wednesday Slide Conference, 2025-2026, Conference 8, Case 2
Signalment:
11-month-old Toy Poodle, Female SpayedHistory:
The patient presented for left hindlimb lameness which was localized to the left hip. Radiographs were most consistent with a diagnosis of Legg–Calvé–Perthes disease. The patient underwent a femoral head osteotomy, and the tissue was submitted for histopathology.Gross Pathology:
IMAGE ONLY WITH CAPTION - A photograph of the femoral head taken immediately post operatively. The femoral head is misshapen with a focal region of flattening and indentation adjacent to the ligamentum capitis femoris. Orientation was not provided with the gross image.Laboratory Results:
IMAGE ONLY WITH CAPTION - Pre-operative VD radiograph of the hips showing bone loss, osteolysis and a severely misshapen left femoral head.Microscopic Description:
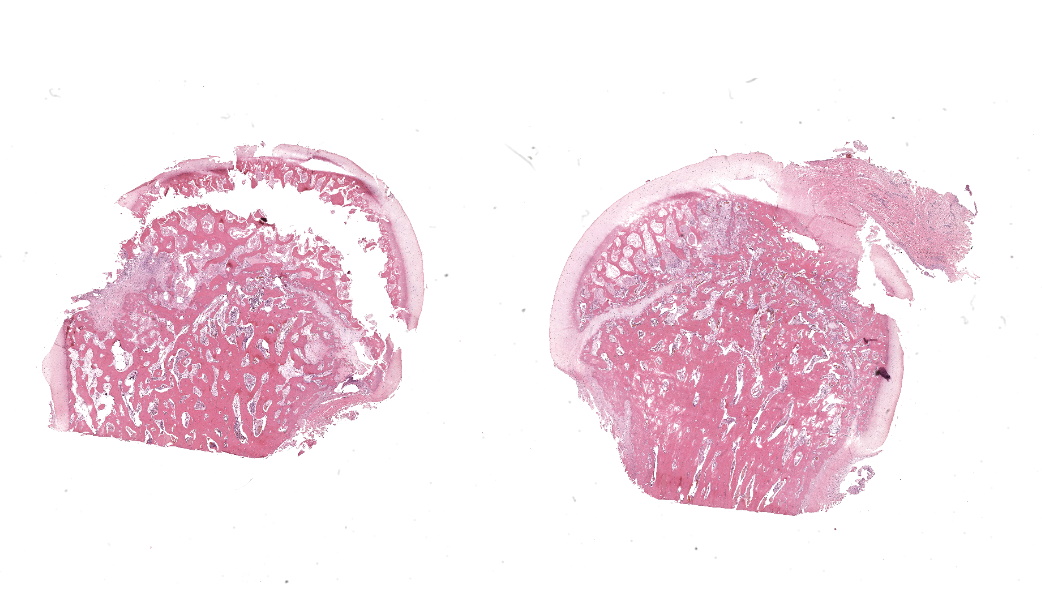
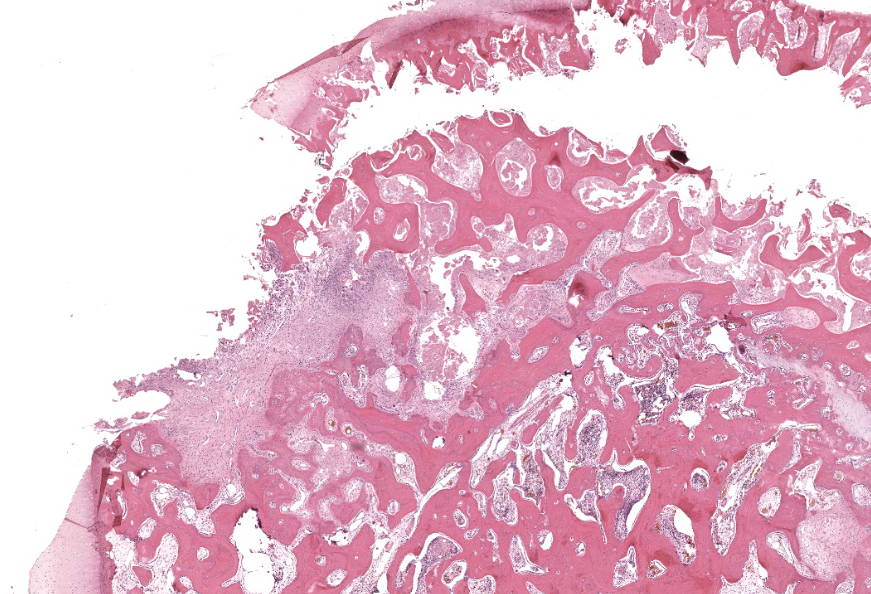
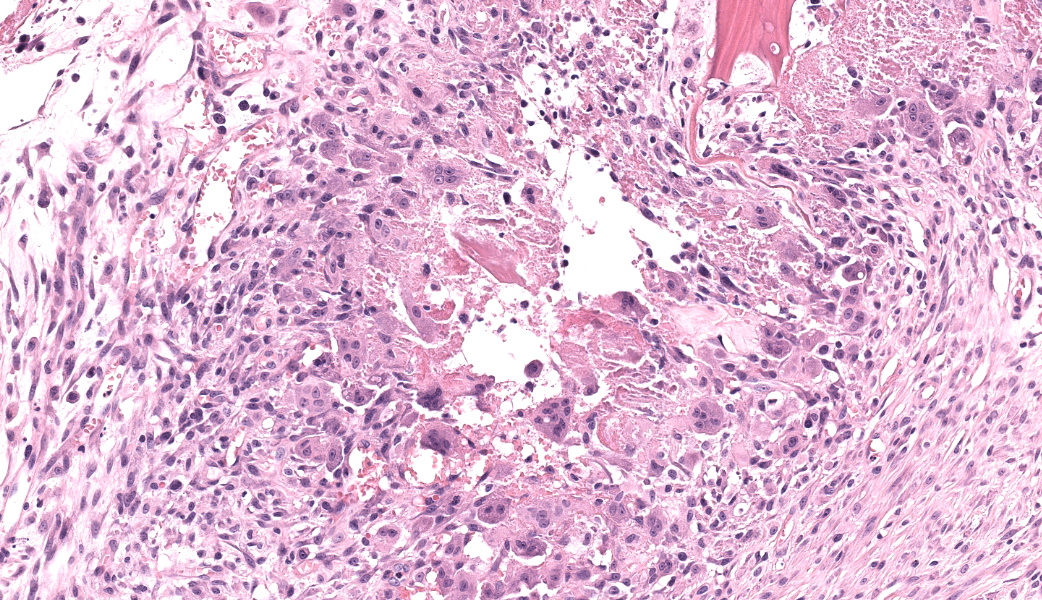
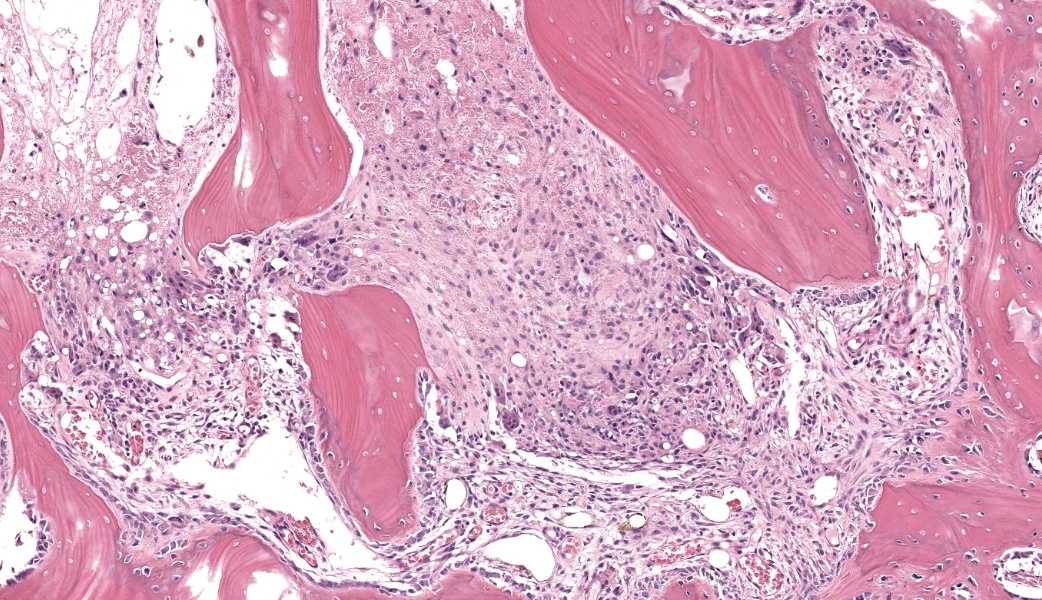
Femoral head: Affecting approximately 30-50% of the epiphysis from the subchondral aspect of the articular cartilage to the physis, there is a focally extensive area of osteonecrosis characterized by bony trabeculae which are irregular and brightly eosinophilic with loss of differential staining. There is loss of both osteocytes within lacunae and osteoblasts lining trabeculae in this region. Along the margins of the necrotic area, multiple bone trabeculae are fragmented and/or have scalloped margins with osteoclasts in Howship’s lacunae (osteolysis). The intertrabecular spaces within and at the periphery of the necrotic area contain variably amounts of amorphous eosinophilic matrix (fibrin), occasional neutrophils and macrophages and/or loosely arranged myxomatous to collagenous matrix with variable numbers of plump spindle cells and capillaries (fibroplasia). Occasionally, there are also finer, irregular trabeculae of paler staining or partially mineralized bone (woven bone). Adjacent viable trabeculae are lined by numerous active osteoblasts (remodeling) and are sometimes laced with wavy basophilic lines (resting / resorption lines). The articular cartilage is fragmented (likely artefact).Contributor's Morphologic Diagnoses:
Osteonecrosis, focally extensive, chronic with fibroplasia and bone remodeling; femoral head.Contributor's Comment:
The signalment, clinical history, radiographic findings and histopathology are most consistent with a diagnosis of avascular necrosis of the femoral head, also known as Legg-Calvé-Perthes Disease or Osteonecrosis of the femoral head.Avascular necrosis of the femoral head (ANFH) is a well-recognized condition which occurs most frequently in small breed dogs, including miniature poodles, West Highland White terriers and Yorkshire terriers.3 This condition is heritable in these breeds and there is evidence to support an autosomal recessive mode of inheritance.2,3 Most affected individuals present between 3 and 13 months of age with unilateral hindlimb lameness.2 The condition is bilateral in approximately 12-17% of cases.2 A significant percentage of dogs have concurrent patellar luxation which can complicate diagnosis, particularly as radiography lacks sensitivity in detecting early cases.2,7
ANFH is not always a heritable condition. In humans and dogs ANFH can be broadly categorized as non-traumatic or traumatic, and within those categories, as pediatric or adult.5 Traumatic cases are typically associated with femoral neck fractures; this should be excluded clinically in affected dogs.3,5 In humans, although most ‘non-traumatic’ cases of ANFH are deemed idiopathic, there is typically some metabolic disorder which underpins the disease, with alcoholism and steroid administration among the most common in adults.5 A number of experimental animal models have examined the pathophysiology of osteonecrosis because there remains no consensus on an optimal approach for treatment in humans.4
Although ANFH is often labelled ‘idiopathic’, it is well understood that vascular compromise and subsequent ischemia of the bone are involved in the pathogenesis in both humans and animals.3,4,5,6 The underlying cause or trigger of vascular compromise is varied, particularly in affected human adults with underlying metabolic disease.5 In young, small breed dogs with heritable ANFH it is postulated that the development of the vascular supply of the femoral head contributes to the condition.3 In normal, crossbred dogs the blood vessels supplying the femoral head are gradually incorporated into fibro-osseous canals during development and as such are well protected by the surrounding bone.3 In Miniature poodles, which are highly susceptible to the heritable, juvenile form of ANFH, the incorporation of these vessels is delayed or does not occur completely.3 As a result, even a slight increase in intraarticular pressure can result in venous occlusion and subsequent ischemic injury.3 Joint effusion due to transient episodes of synovitis or minor trauma could trigger the condition in predisposed individuals.2,3
The gross and microscopic pathology varies depending on the chronicity of the disease at the time of diagnosis.1,3 Early on, the shape and structure of the femoral head are grossly and radiographically normal. Histologically, there may be evidence of osteonecrosis predominantly within the subchondral bone at this stage.1 With chronicity, if the area of necrosis is large enough, the necrotic bone collapses which causes flattening of the femoral head (Figure 1) which eventually results in a degenerative arthropathy.1,3
Contributing Institution:
Murdoch University Pathology Services. www.murdoch.edu.auJPC Diagnoses:
Femur, epiphysis: Osteonecrosis, chronic, focally extensive, moderate, with osteolysis, woven bone, fibrosis, and bony remodeling.JPC Comment:
The contributor of this case gives an excellent overview of this condition.Most of conference discussion was centered on pathogenesis and key histologic features of this condition. This disease can be, as stated by the contributor, either hereditary or secondary to trauma or other ischemic event.1,3,4,5,6 The hereditary form is most often seen in young, small breed dogs, such as terriers, dachshunds, pugs, Chihuahuas, and toy poodles. When looking at this case, there are a few histologic clues that can assist in determining the age of this animal, which can help with reaching the correct diagnosis. These include the presence of discontinuous physeal cartilage and the horizontal orientation of the bony spicules deep to the physis. In dogs, physes typically close around 10 months of age. Physis closure in Legg-Calves-Perthes disease (LCPD) is typically delayed secondary to ischemia of the physeal cartilage and the subchondral bone, which can result in a malformed or improperly angled femoral head.1 Additionally, in young animals, the bony spicules that extend into the metaphysis from the developing stages of the growth plate are oriented vertically (perpendicular) to the growth plate to facilitate the elongation of the bone. In older animals that have closed physes, the bone below the growth plate becomes oriented horizontally (parallel) to the growth plate, effectively “capping” it to facilitate closure of the physes. In this case, the bone has become horizontally oriented below the growth plate, indicating that this animal should have closed physes at this stage, but the presence of and discontinuity of the lingering growth plate indicate that this young animal is likely experiencing delayed physeal closure.
There are three recognized grades of LCPD and include: Grade 1, defined as necrosis of bone with empty lacunae, lack of viable bone marrow, and normal articular chondrocytes.
Grade II, characterized by cracks in the articular cartilage, subchondral bone collapse, and flattening of the femoral head with re-vascularization coming in from the periphery of the epiphysis +/- granulation tissue development; and Grade III, in which the articular cartilage is highly deformed with folds and cracks and the femoral head loses its shape.1
In the early stages (Grade I) of LCPD, the articular cartilage is spared because of its avascular nature.1,3,5 The subchondral bone, however, will become necrotic, and there is frequently a characteristic “tideline” of hypereosinphilia between the unaffected articular cartilage and the affected subchondral bone.3,5 As the condition progresses, however, the joint is subjected to altered conductive forces from abnormal weight-bearing, which places excessive pressure upon the articular surface and ultimately results in articular cartilage loss.1,5 This results in both the flattening of the femoral head from mechanical collapse and in asymmetrical growth between the affected limb and unaffected limb, as this disease is usually unilateral.5 Additionally, secondary to the altered conductive forces through the joint, new woven bone begins proliferating in an attempt to re-stabilize the bone and adjust for the altered force conduction.1 This woven bone is usually seen flanking either side of an area of lamellar bone to create a “sandwich” effect.
Differentiating necrotic bone from normal bone can be challenging, but one of the key features to look for is the loss of osteocytes from lacunae.5 Osteocytes either become pyknotic and hypereosinophilic or disappear entirely, and you can best convince yourself this is a real change (and not just a staining artifact) by comparing an area of suspected necrosis to an area of less affected or normal bone where the osteocytes will still be in their lacunae and have a nice, basophilic nucleus. Another useful way to determine osteonecrosis is to assess the bone marrow. In necrotic bone, there is usually histologic loss of marrow elements secondary to ischemia, which will manifest as a loss of differential staining with retention of architecture within the marrow.
References:
- Aguado E, Goyenvalle E. Legg Calvé Perthes disease in the dog. Morphologie. 2021;105:143-147.
- Cardoso CB, Rahal SC, Mamprim MJ, Oliveira HS, Merlchert A, Coris JGF, dos Reis Mesquita L. Avascular necrosis of the femoral head in dogs-retrospective study. Acta Scientiae Veterinariae. 2018;46:5-5.
- Craig LE, Dittmer KE, Thompson KG. Bones and joints. Jubb, Kennedy & Palmer’s pathology of domestic animals. 2015;1:16-163.
- Fan M, Peng J, Qin L, Lu S. Experimental animal models of osteonecrosis. Rheumatology International. 2011;31:983-994.
- Guerado E, Caso E. The physiopathology of avascular necrosis of the femoral head: an update. Injury. 2016;47:S16-S26.
- Kerachian MA, Harvey EJ, Cournoyer D, Chow TY, Séguin C. Avascular necrosis of the femoral head: vascular hypotheses. Endothelium. 2006;13:237-244.
- Mapuvire T. Legg-Calvé-Perthes Disease in the Dog: A Case-Based Review. South African Veterinary Association. 2023.
- Vasseur PB, Foley P, Stevenson S, Heitter D. Mode of inheritance of Perthes' disease in Manchester terriers. Clinical Orthopaedics and Related Research. 1989;244:281-292.