Signalment:
Gross Description:
Histopathologic Description:
Morphologic Diagnosis:
Condition:
Contributor Comment:
With eosinophilic granulomas, single or multiple lesions, ranging from 0.5 to 10 cm in diameter, are most commonly found on the withers and back, but can also be seen in the girth area, the mane, the rump, and the face. The lesions are often round, firm, and well-circumscribed with no ulceration or alopecia. Pain and pruritus are not present. Some lesions can be cystic or plaque-like with a central caseous core.(4,5)
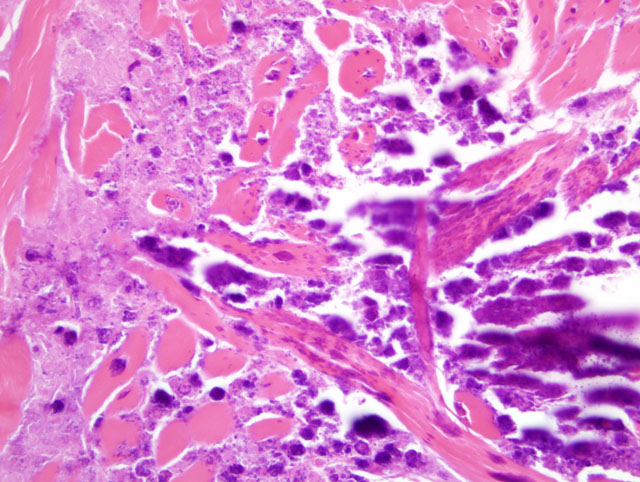
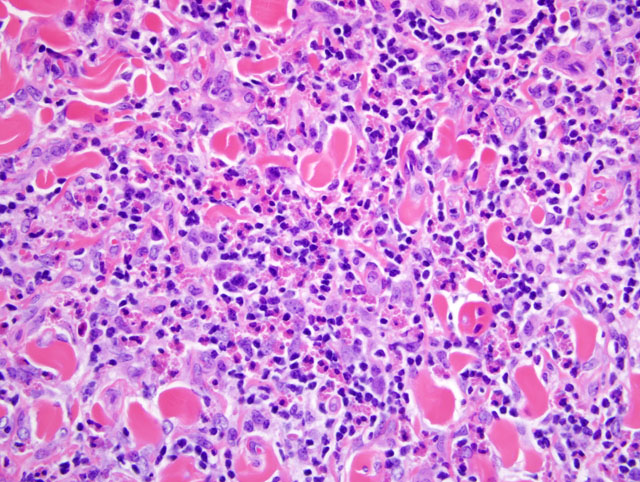
Massive central necrosis consisting of degranulating, degenerative eosinophils is a key element of this lesion.(6) The amount of collagenolysis varies among lesions. To date, the reason for the absence of collagenolysis in some lesions is not known. Collagen degeneration has been hypothesized to be the result of toxic products derived from degranulating eosinophils, such as major basic protein.(6) Some more chronic lesions can present with dystrophic mineralization and thus be misdiagnosed as calcinosis circumscripta or tumoral calcinosis.(5)
Histologically, the lesions of nodular collagenolytic granulomas (eosinophilic granulomas) need to be differentiated from those of habronemiasis and hypoderma nodules.(7) Cutaneous habronemiasis (summer sores) is caused by the larval activity of three nematodes that inhabit the horses stomach, especially Draschia megastoma, during the summer months. The larvae are deposited on the skin by flies, which are attracted to a pre-existing wound. Lesions are particularly common in the skin of the pectoral region, between the forelegs. The larvae penetrate deeply into the dermis and elicit an eosinophilic and granulomatous response. The alopecic ulcerated skin becomes encrusted by a serous exudate that oozes from the surface.(3) In hypodermiasis, by contrast, there is the presence of a breathing pore for the parasite. Cutaneous habronemiasis was considered as the primary differential diagnosis; however, due to the absence of larvae in the sections, the lack of skin ulceration and alopecia, and the presence of degenerate collagen, eosinophilic granuloma (nodular collagenolytic granulomas) was diagnosed.Â
JPC Diagnosis:
Conference Comment:
1. Perivascular dermatitis
2. Interface dermatitis
3. Vasculitis
4. Nodular and diffuse dermatitis
5. Intraepidermal vesicular and pustular dermatitis
6. Subepidermal vesicular and pustular dermatitis
7. Perifolliculitis, folliculitis, and furunculosis
8. Fibrosing dermatitis
9. Panniculitis
10. Atrophic dermatitis
In addition to the entities well-described by the contributor (i.e. eosinophilic granuloma, habronemiasis, and hypodermiasis), the differential diagnosis for eosinophilic dermatitis in horses includes mast cell tumor, cutaneous pythiosis, multisystemic eosinophilic epitheliotropic disease, sterile eosinophilic folliculitis and furunculosis, unilateral papular dermatosis, and axillary nodular necrosis. For most of these, differentiation from eosinophilic granuloma is relatively straightforward; however, axillary nodular necrosis and unilateral popular dermatosis bear many histomorphologic similarities to eosinophilic granuloma, often creating a diagnostic challenge. These conditions were discussed at length, and their key features are summarized in the table below:(1,5)
| Condition | Clinical and Gross Findings | Histomorphology |
| Eosinophilic granuloma (nodular necrobiosis, collagenolytic granuloma) | Most common equine cutaneous eosinophilic nodular disease; 0.5-10 cm diameter nodules anywhere on the body (often withers and back); trauma or hypersensitivity to insect bites or silicone coating on needles suspected | Dermal collagen flame figures surrounded by eosinophilic granulomatous inflammation; +/- eosinophilic folliculitis or furunculosis; +/- dystrophic mineralization; +/- lymphoid follicles; true collagen degeneration is rare |
| Axillary nodular necrosis | Usually unilateral; few (3-10) cutaneous and subcutaneous, 1-10 cm diameter nodules; truncal, caudal to axilla ("girth galls") | Eosinophilic coagulative necrosis surrounded by eosinophilic granulomatous dermatitis and panniculitis; dermal collagen flame figures; dystrophic mineralization of collagen; lymphoid nodules; eosinophilic or necrotizing vasculitis with endothelial cell hypertrophy, vessel lumen occlusion, and intimal mucinosis |
| Unilateral papular dermatosis | More common in spring and summer; Quarter Horses over-represented; numerous (30 to 300) unilateral, truncal, 2-10 mm diameter cutaneous nodules and papules; ectoparasite hypersensitivity suspected | Eosinophilic folliculitis and furunculosis; eosinophilic dermal inflammation; +/- dermal collagen flame figures |
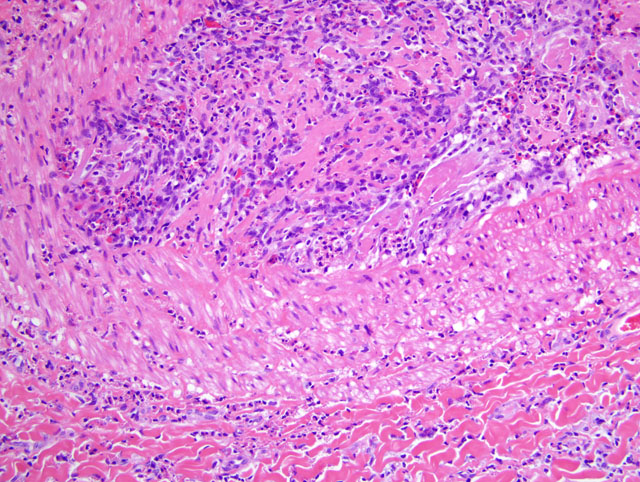
While the anatomic location is most consistent with eosinophilic granuloma, the vascular lesions observed by several conference participants in this case are strongly suggestive of axillary nodular necrosis. Throughout the deep dermis, all arterioles contain abundant, pale, basophilic, finely-granular subendothelial material (intimal mucinosis). Additional histologic findings present in some sections include hair shafts embedded in the deep dermis, recanalization of the thrombus in a large arteriole, few lymphocytes and plasma cells in the superficial dermis and periadnexally, and mild acanthosis, spongiosis, and orthokeratotic hyperkeratosis of the overlying epidermis.Â
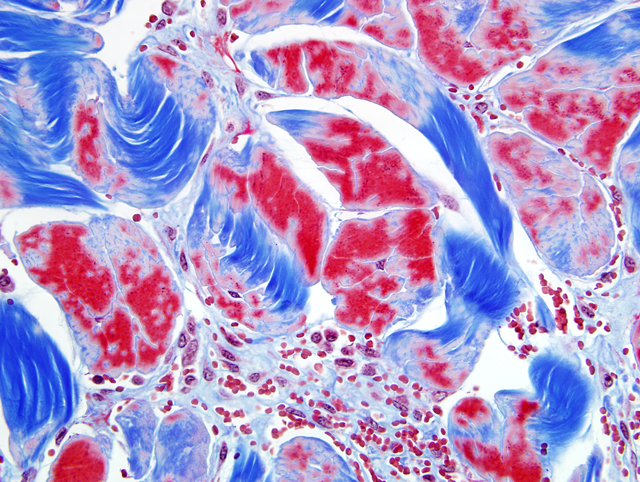
Finally, conference participants discussed the terms collagenolysis and flame figure. Collagenolysis or collagen necrobiosis, which implies true collagen degeneration, is the term classically used for the characteristic intense, acellular, eosinophilic material centered on collagen fibers in a variety of eosinophilic dermatoses. However, in many of these conditions Massons trichrome staining and ultrastrucutural examination are inconsistent in demonstrating true collagen degeneration. Often, abnormal (i.e. red) staining of collagen fibers with Massons trichrome is as likely to be present in areas of eosinophil degranulation as it is in other, apparently unaffected areas of the tissue section; therefore, many prefer the term flame figure to describe the histologic features, particularly when true collagen degeneration cannot be definitively demonstrated. In this case, Massons trichrome staining revealed abnormal, red-staining collagen cores in over 90% of the dermal collagen bundles, but not areas containing flame figures. Major basic protein from degranulating eosinophils is now thought to be the source of the intense eosinophilic material seen in flame figures.(2)
References:
2. Gross TL, Ihrke PJ, Walder EJ, Affolter VK: Skin Diseases of the Dog and Cat: Clinical and Histopathologic Diagnosis, 2nd ed., pp. 356-357. Blackwell Publishing, Ames, IA, 2005
3. Jones TC, Hunt RD, King NW: Veterinary Pathology, 6th ed., pp. 639. Williams and Wilkins, Baltimore, MD, 1997
4. Mathison PT: Eosinophilic nodular dermatoses. Vet Clin North Am Equine Pract 11:75-89, 1995
5. Scott DW, Miller WH: Equine Dermatology, pp. 647-667. Saunders Elsevier, St. Louis, MO, 2003
6. Slovis NM, Watson JL, Affolter VK, Stannard AA: Injection site eosinophilic granulomas and collagenolysis in 3 horses. J Vet Intern Med 13:606-612, 1999
7. Yager JA, Scott DW: The skin and appendages. In: Pathology of Domestic Animals, eds. Jubb KVF, Kennedy PC, Palmer N, 4th ed., vol. 1, pp. 700-701. Academic Press, San Diego, CA, 1993