Signalment:
Three-year-old,
male, English setter mix, (
Canis familiaris).The
three-year-old intact male English setter mix was picked up by county animal
control when it was found roaming freely in a small rural community in Southern
Arizona. Aspirate cytology from the preputial mass and several cutaneous
masses were submitted.
Gross Description:
The dog
had a large ulcerated circumferential mass effacing the preputial mucosa and
numerous variably sized cutaneous masses throughout the caudal dorsum, right
and left flank, and inguinal regions. The superficial cervical lymph nodes
were enlarged.
Histopathologic Description:
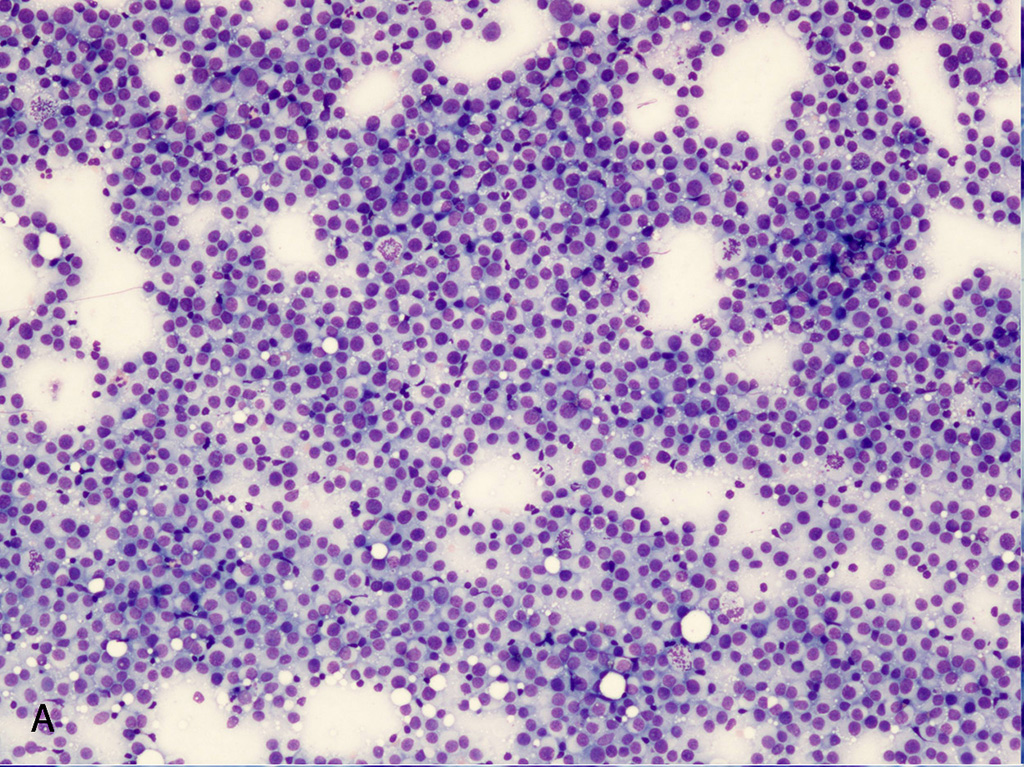
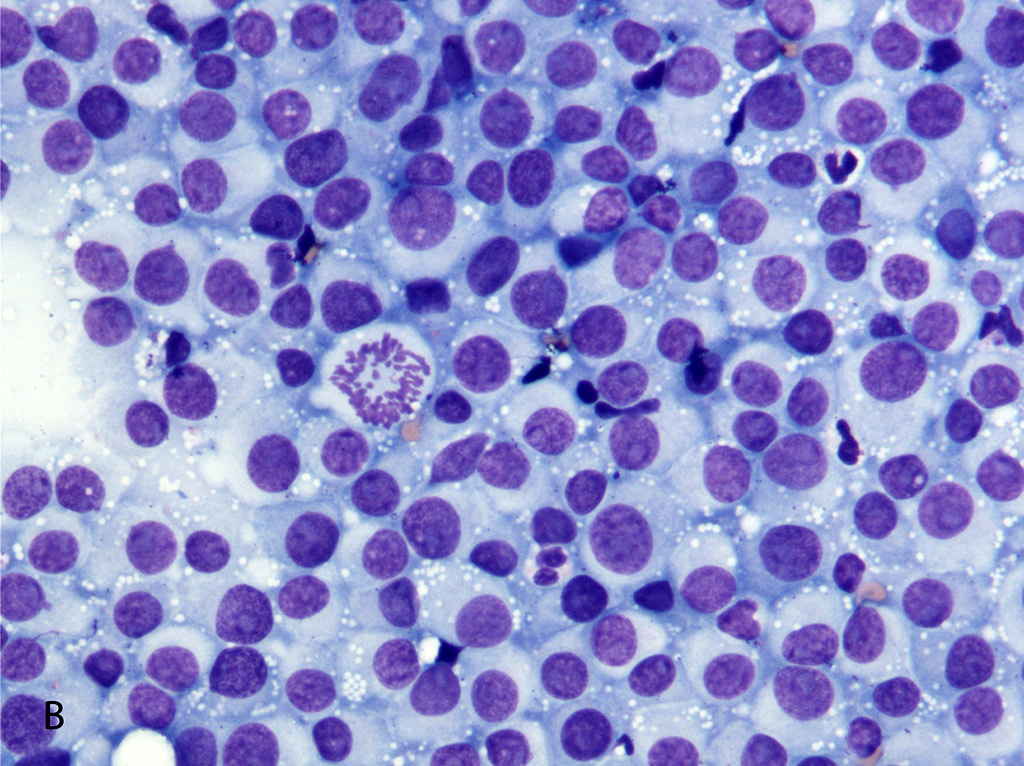
The aspirate preparations from the dermal masses all revealed the same
process. The preparations have high cellularity with large numbers of intact
cells for evaluation. There is minimal hemodilution. The nucleated cell
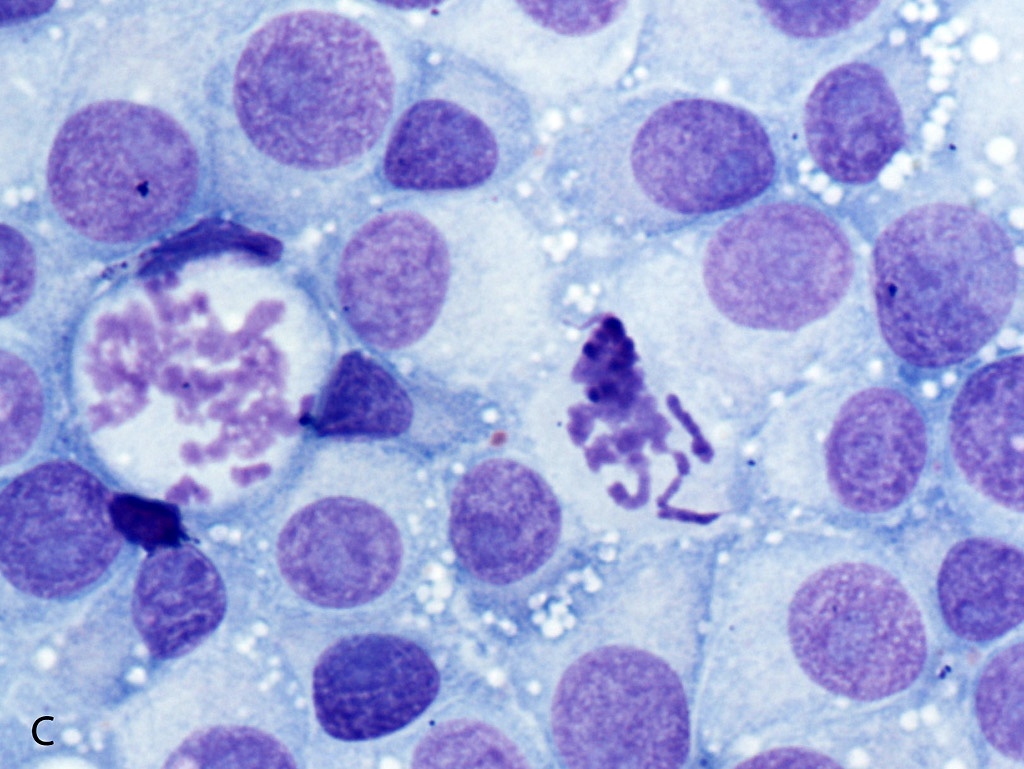
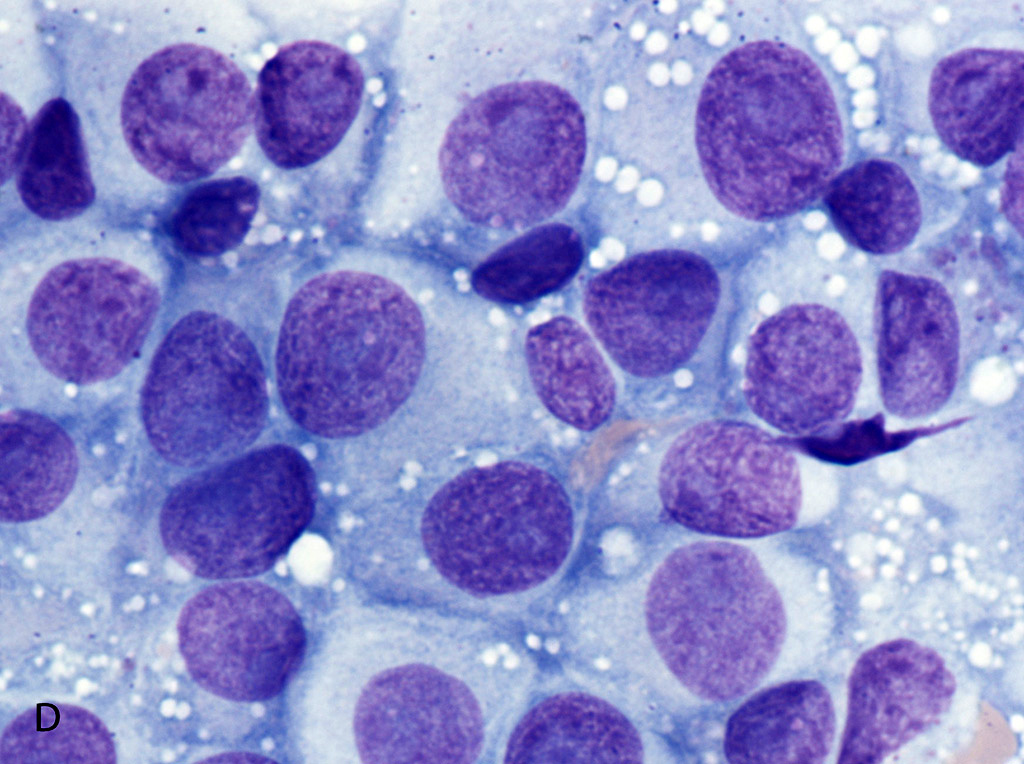
population consists of round cells with moderate anisokaryosis and
anisocytosis. The nuclei are round with coarse ropey chromatin and often
have a single large pale lightly basophilic nucleolus. The cytoplasm is lightly
basophilic and contains small to moderate numbers of discrete round vacuoles.
Mitotic figures are common and atypical mitoses are seen. There are occasional
neutrophils and small lympho-cyte seen intermixed with the neoplastic round
cells. The cytology
preparations from the prepuce showed the same cytological findings.
Morphologic Diagnosis:
Transmissible venereal tumor (TVT) metastatic to skin.
Lab Results:
The dog was
positive for
Ehrlichia canis using in-house ELISA testing.
Condition:
Transmissible venereal tumor
Contributor Comment:
Transmissible venereal tumor is a transplantable neoplasm that affects members
of the canid family (domestic dogs, coyotes, foxes, and wolves).
3
The tumor has a global distribution and highest prevalence in regions with
limited canine population control. The tumor spreads by sexual contact and is
usually localized to the mucosal surface of the external genitalia of both male
and female dogs. However, masses have been reported in the mucosal surfaces of
the nasal passage, oral mucosa, anus, and conjunctival surfaces of the eye.
3,7
Metastatic disease is not common but has been documented. In most cases,
metastasis is to the regional lymph nodes, but extension of the neoplasm to
skin, kidney, brain, bone, peritoneum, and other tissues has been reported.
1,3
The tumor cells are aneuploid and have a unique long interspersed nuclear
element (LINE-1) that may be useful to confirm TVT origin in cases involving
tumors in unusual sites.
10,12
While
TVT is a relatively uncommon tumor in most of the United States, rural areas
that have higher numbers of intact dogs, such as many parts of Southern
Arizona, cases are seen on a regular basis. The histological and cytological
characteristics of the neoplastic cells along with the location of the mass in
association with the external genitalia make the diagnosis of this tumor
relatively straight forward. In this case, the cytological and histological
findings from the skin lesions and the preputial lesion were identical
supporting metastatic disease. There is one report of a prepubertal female dog
without any genital involvement.
4 It is proposed that the tumor
cells were transplanted from the dam by cohabitation and grooming/social
behaviors. While multicentric disease cannot be ruled out, it is unlikely that
multiple sites of transplantation through intact haired skin would explain the
presence of the skin lesions in this adult male dog with a concurrent preputial
mass.
JPC Diagnosis:
Fine
needle aspirate, cutaneous mass: Transmissible venereal tumor, English setter
mix,
Canis familiaris.
Conference Comment:
Canine trans-missible venereal
tumor (TVT), also known as Sticker tumor or venereal granuloma, is an extremely
old and remarkably stable transmissible cancer that first arose in canids
approximately 11,000 years ago.
2,5 Based on genetic studies, the
founder breed is thought to be closely related to wolves or ancient Eastern
Asian dog breeds.
1 TVT dispersed across several continents about 500
years ago and is currently found on every continent in the world other than
Antarctica.
5,12 It is the oldest known continuously passaged somatic
cell lineage.
5 As mentioned by the contributor, TVT is mainly
transmitted during coitus, but can also be transmitted by licking, biting, or
rubbing behaviors.
2,8 The infecting cells are physically
transplanted and grow as a xenograft in host tissue. Neoplastic cells are
thought to be of histiocytic origin and are immune-positive for vimentin,
lysozyme, alpha-1-antitypsin, glial fibrillary acidic protein, and are
immune-negative for cytokeratin, S100, and muscle markers.
1,2,9
Typical gross findings of TVT include solitary or
multiple papillary, nodular, ulcerated, and inflamed masses on the mucous
membranes of the penis, prepuce, vulva, and vagina, and/or skin and subcutis of
the head, neck, limbs, trunk, scrotum, and perineum. There is occasional extension
to the uterus and cervix.
2,9 A recent study demonstrated ocular
lesions as the single manifestation of TVT with extension to the adjacent
conjunctiva and nictitating membrane, presumably by extra-genital inoculation.
3
As mentioned by the contributor, metastasis uncommonly occurs in the draining
lymph node.
9
After transmission, tumorous lesions typically appear within
two months. Conference participants discussed the patho-genesis of the tumor
growth, stabilization, and regression phases. The initial growth stage is
called the progressive phase (P). During the P phase, almost all TVT cells lack
expression of major histocompatibility complex (MHC) I and II due to production
of inhibitory cytokine transforming growth factor-beta (TGF-beta). This allows
the TVT cells to grow and evade immune destruction by cytotoxic T-lymphocytes. After three to
nine months, the tumor stabilizes and begins to spontaneously regress. During the regression (R) phase, interleukin-6 (IL-6) from
infiltrating lymphocytes is thought to work in conjunction with
interferon-gamma (IFN-gamma) to antagonize TGF-beta and increase MHC I and II
expression on TVT cells.
1,8-10
In addition to TVT, conference participants also discussed
the devil facial tumor disease (DFTD), which is an emerging rapidly fatal
transmissible tumor that is decimating the wild Tasmanian devil population.
8,11
This tumor is of Schwann cell origin and is spread through biting. Tumors occur
primarily in the mouth, head, and neck. DFTD cells evade immune destruction via
production of TGF-beta and down regulation of MHC-I and II expression, similar
to TVT. However, unlike TVT, spontaneous regression has not been reported in
DFTD, and mortality occurs in all affected animals via starvation and frequent
metastasis.
8 Other transmissible tumors include clam leukemia of
soft shell clams and the contagious reticulum cell sarcoma of Syrian hamsters
first described in the 1960s.
6,8,11
References:
1. Ganguly B, Das U, Das AK. Canine transmissible venereal
tumor: A review.
Comp Oncol. 2016; 14(1):1-12.
2. Gross TL, Ihrke PJ, Walder EJ, Affolter VK.
Skin Diseases
of the Dog and Cat. 2nd ed. Oxford, UK: Blackwell Publishing; 2005:800-803.
3. Komnenou AT, Thomas AL, Kyriazis AP, et al. Ocular
manifestations of canine trans-missible venereal tumor: A retrospective study
of 25 cases in Greece.
Vet Rec. 2015; 176(20):523-527.
4. Marcos R, Santos M, Marrinhas C, et al. Cutaneous
transmissible venereal tumor without genital involvement in a prepubertal
female dog.
Vet Clin Pathol. 2006; 35:106109.
5. Murchison EP, Wedge DC, et al. Transmissible dog cancer
genome reveals the origin and history of an ancient cell lineage.
Science.
2014; 343:437-440.
6. Ostrander EA, Davis BW, Ostrander GK. Transmissible tumors:
Breaking the cancer paradigm.
Trends Genet. 2016; 32:1-15.
7. Park MS, Kim Y, Kang MS, et al., Disseminated transmissible
venereal tumor in a dog.
J Vet Diagn Invest. 2006; 18(1):130-133.
8. Pye RJ, Woods GM, Kreiss A. Devil facial tumor disease.
Vet
Pathol. 2016; 53(4):726-736.
9. Schlafer DH, Foster RA. Female genital system. In: Maxie MG,
ed.
Jubb, Kennedy, and Palmers Pathology of Domestic Animals. Vol 3.
6th ed. St. Louis, MO: Elsevier; 2016:448-449.
10. Setthawongsin
C, Techangamsuwan S, Tangkawattana S, et al. Cell-based polymerase chain
reaction for canine transmissible venereal tumor (CTVT) diagnosis.
J Vet Med
Sci. 2016; 78(7):1167-1173.
11. Siddle
HV, Kaufman J. A tale of two tumours: Comparison of the immune escape
strategies of contagious cancers.
Mol Immunol. 2013; 55:190-193.
12. VonHoldt
BM, Ostrander EA. The singular history of a canine transmissible tumor.
Cell.
2006; 126(3):445-447.
1.