Signalment:
2008.3.25 This cat showed diarrhea lasting for one month and gradual weight loss for one year from 4.82kg to 3.76kg. Diarrhea disappeared immediately after general treatment with an anti-diarrheal drug.
2008.5.12 Repeated vomiting appeared from recent two weeks with complete loss of appetite. A mass lesion was found in the abdominal cavity by X-ray examination and echography.
2008.5.13 Intestinal obstruction was confirmed in the small intestine by barium contrast study.
2008.5.14 The mass was surgically removed. The enlargement of the mesenteric lymph node was observed during a laparotomy.
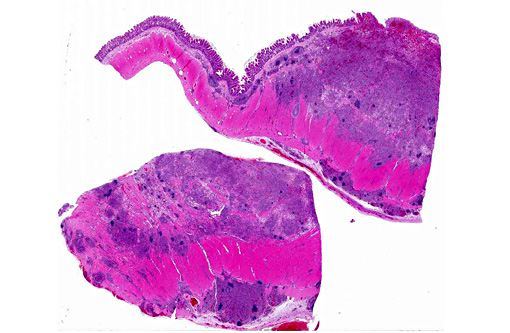
Gross Description:
Histopathologic Description:
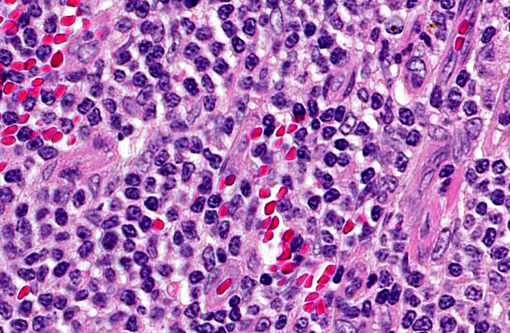
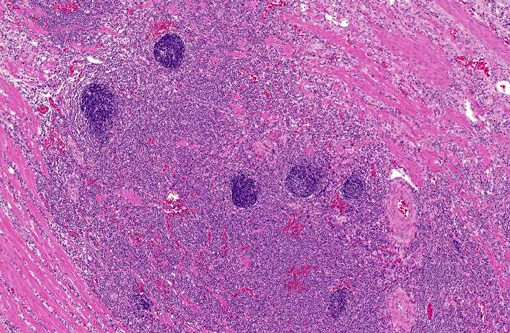
Immunohistochemically, the majority of tumor cells were positive for CD3 and TIA-1, negative for CD79a and CD20. In the muscular layer where the lymph follicles formed, many cells forming the follicles were positive for CD79a and CD20 and negative for CD3 and TIA-1, whereas a few cells of germinal center were positive for CD3 and TIA-1.
Based on immunohistochemical findings, tumor cells have a T-cell phenotype in this lymphoma but lymph follicles formed in the tumor mass consisted of B-cells.
Morphologic Diagnosis:
Lab Results:
Condition:
Contributor Comment:
The present case was characterized by formation of lymph follicles in the mass of tumoral proliferation. These lymph follicles were not original lymphoid tissue, because they were formed in muscular and serosal layers where there is no lymphatic tissue in the normal condition. In addition, this lymphoma had a T-cell phenotype and the follicles were composed of B-cell phenotype. Therefore, it was likely that lymphoid follicles were formed due to the reactive response to tumor cells or immunologic stimuli by the altered environment resulting in proliferation of tumor cells. The neoplastic cell proliferation forming lymph follicles was similar to lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma) in morphologic growth pattern. MALT lymphoma and marginal zone lymphoma are B-cell lymphoma,(14) and the tumor cells encircle follicles outside the mantle cell layer in these types of lymphoma. Cytologically, T-cell lymphoma consists of smaller cells with low mitotic rate as in the present case. However, MALT lymphoma is usually composed of small lymphocytes with indented nuclei, or there may be a more mixed pattern with some larger lymphoid cells similar to the centrocytes and centroblasts of benign germinal centers.(14)
Intestinal T-cell lymphoma is characterized also by epitheliotropism of tumor cells.(2,8,15) Neoplastic lymphocytes usually are small round cells that resemble mature lymphocytes. However, epitheliotropism was not seen in the tumor cells of the present case. In a report of canine intestinal T-cell lymphoma, approximately 25% did not show epitheliotropic behavior.(14) In addition, in humans, MALT lymphoma usually forms lymphoepithelial lesions and tumor cells invade between mucosal epithelium. Lymphoepithelial lesions resemble epitheliotropism, but are characterized by centrocyte-like cell invasion and destruction of the epithelium. Therefore, epitheliotropism is not specific for T-cell lymphocytes and formation of lymph follicles is also not specific for B-cells.
JPC Diagnosis:
Conference Comment:
The most common presentation of lymphoma in cats has evolved as the success of FIV/FeLV testing and vaccination programs have been realized. In the 1970s, 70% of feline lymphoma cases in the U.S. were attributed to FeLV infection which dropped to less than 15% twenty years later.(1) Interestingly, as the prevalence of these known oncogenic viruses have diminished, the incidence rate of lymphoma in cats appears to be increasing.(1,9) Retroviral-associated lymphomas commonly presented as mediastinal or multicentric forms in young cats.(3,12) The majority of lymphomas in cats now occur in the gastrointestinal tract.(9) Recent literature has also described a shift in prevalence from B-cell to T-cell lymphomas in intestinal lymphoma in cats.(9,12) Diffuse large B-cell lymphomas are considered most common in the stomach of cats.(9) Other subclassifications of significance in cats include large granular lymphocyte lymphoma which also occurs in the intestinal tract but often with more systemic involvement and is associated with a poor prognosis. T-cell rich large B-cell lymphoma is an indolent type with a mixed cell population to include bizarre giant or multinucleated cells and typically presents in a single lymph node.(3)
Conference participants were interested in the unique histologic presentation of lymphoma in this case, with the formation of multiple lymphoid follicles dispersed throughout all levels of the muscularis mucosa. Theories regarding their formation were exchanged, including immune stimulation by antigens or toxin absorption through the disrupted mucosal epithelium.
References:
1. Beatty J. Viral causes of feline lymphoma: retroviruses and beyond. Vet J. 2014;201:174-180.
2. Carreras JK, Goldschmidt M, Lanb M, McLear RC, Drobatz KJ, Sorenmo KU. Feline Epitheliotropic intestinal malignant lymphoma: 10 cases(1997-2000). J Vet Intern Med. 2003;17:326-331.
3. Chino J, Fujino Y, Kobayashi T, et al. Cytomorphological and immunological classification of feline lymphomas: clinicopathological features of 76 cases. J Vet Med Sci. 2013;75(6):701-707.
4. Gabor LJ, Canfield PJ, Malik R. Immunophenotypic and histological characterization of 109 cases of feline lymhosarcoma. Austrarian Veterinary Journal. 1999;76:725-736.
5. Gabor LJ, Malik R, Canfield PJ. Clinical and anatomical features of lymphosarcoma in 118 cats. Austrarian Veterinary Journal. 1998;76:725-736.
6. Head KW, Cullen JM, Dubielzig RR, Else RW, Misdorp W, Patnaik AK, et al. Histological classification of alimentary tumors of domestic animals. In: Histological Classification of Tumors of the American System of Domestic Animals. 2nd Series. Vol. X, Washington, DC: Armed Forces Institute of Pathology/ American Registry of Pathology and the Worldwide Reference on Comparative Oncology; 2003:87-100.
7. Head KW, Else RW. Other tumors of the alimentary tract. In: Menten DJ, ed. Tumors in Domestic Animals. Fourth ed. Ames, Iowa: Iowa State Press; 2002:467-8, 471-3.
8. Krecic MR, Black SS. Epitheliotropic T-cell gastrointestinal tract lymphosarcoma with metastasis to lung and skeletal muscle in a cat. J Am Vet Med Assoc. 2000;216:524-529.
9. Moore PF, Rodriguez-Bertos A, Kass PH. Feline gastrointestinal lymphoma: mucosal architecture, immunophenotype, and molecular clonality. Vet Pathol. 2012;49(4):658-668.
10. Ozaki K, Yamagami T, Nomura K, Narama I. T-cell lymphoma with eosinophilic infiltration involving the intestinal tract in 11 dogs. Vet Pathol. 2006;43:339-344.
11. Patterson-Kene JC, Perrins Kugler B, Francis K. The possible prognostic significance of immunophenotype in feline alimentary lymphoma: a pilot study. J Comp Path. 2004;130:220-222.
12. Pohlman LM, Higginbotham ML, Welles EG, Johnson CM. Immunophenotypic and histologic classification of 50 cases of feline gastrointestinal lymphoma. Vet Pathol. 2009;46:259-268.
13. Vail DM. Hematopoietic tumors. In: Ettinger SJ, Feldman EC, eds. Veterinary Internal Medicine. 7th ed. Vol 2. St. Louis, MO: Saunders Elsevier; 2010:2149-2150.
14. Valli VE, Jacobs RM, Parodi AL, Vernau W, Moore PE. Histological classification of hematopoietic tumors of domestic animals. In: Histological Classification of Tumors of the American System of Domestic Animals. 2nd Series, Vol.Ⅷ. Washington, DC: Armed Forces Institute of Pathology/ American Registry of Pathology and the Worldwide Reference on Comparative Oncology; 2002:28-47.
15. Waly NE, Gruffydd-Jones TJ, Stoke CR, Day MJ. Immunohistochemical diagnosis of alimentary lymphomas and severe intestinal inflammation in cats. J Comp Path. 2005;133:253-260.