Wednesday Slide Conference, 2025-2026, Conference 1, Case 1
Signalment:
Equine Standardbred. Female, 2 days.History:
Filly foal born with angular limb deformities of the all limbs, worse in the hind limbs. Foal had a fever, leukocytosis and neutrophilia.Gross Pathology:
The crown rump length of this foal was 112 cm, Bilaterally, the tarsal joints were fixed in extension. The left fetlock has a 15 degree lateral deviation. The right tarsus was deviated about 30% and the fetlock a further 15 degrees medially. Eponychia were on all 4 hooves. The thyroid was normal in appearance. Bone marrow appeared to be normal also.Laboratory Results:
Leukocytosis, neutrophilia, hypoproteinemia, hypoalbuminemia, severe hypoglobulinemia, azotemia, increased bilirubin, cholesterol, GLDH, Alk Phos, and CK.Microscopic Description:
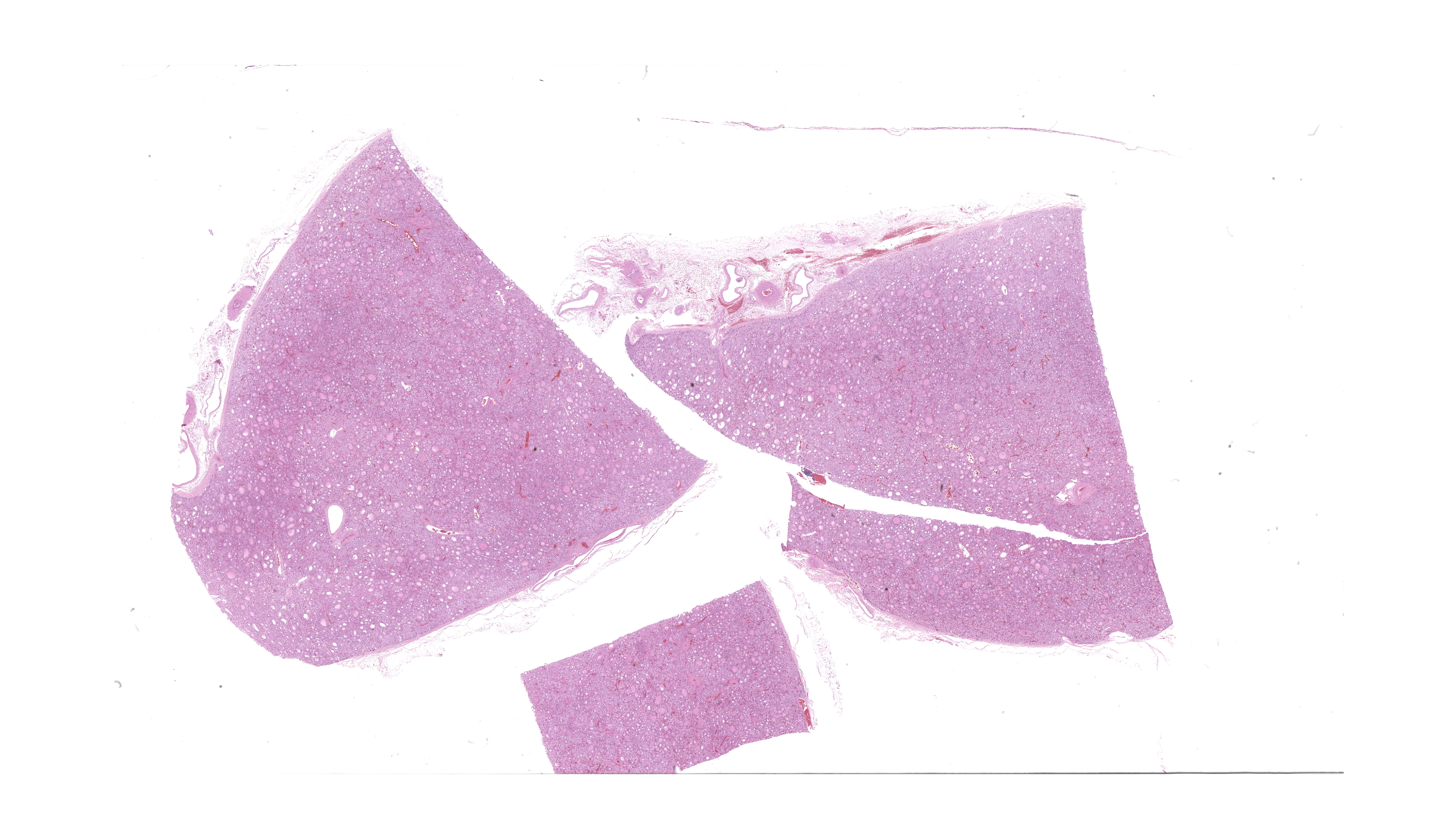
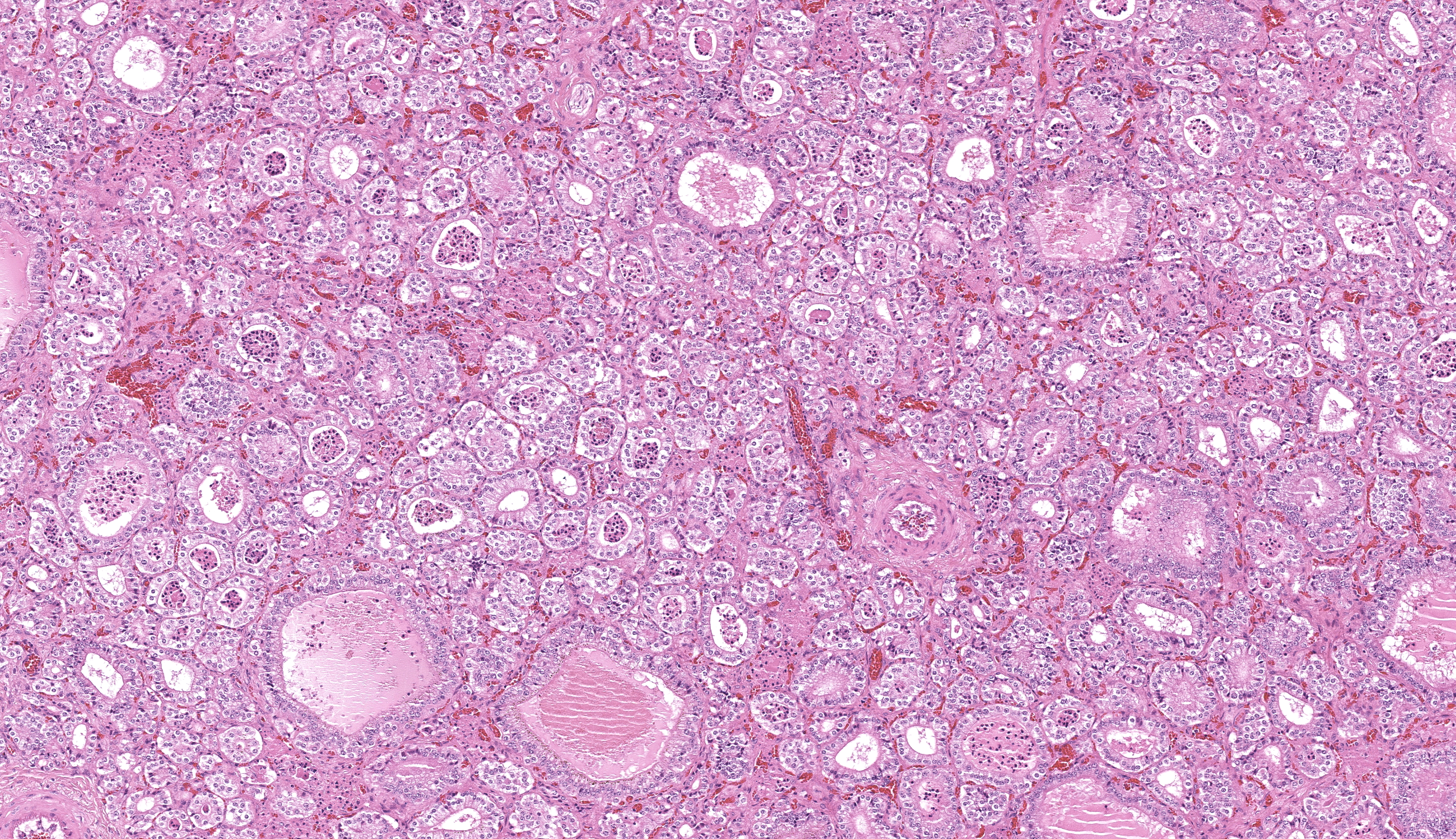
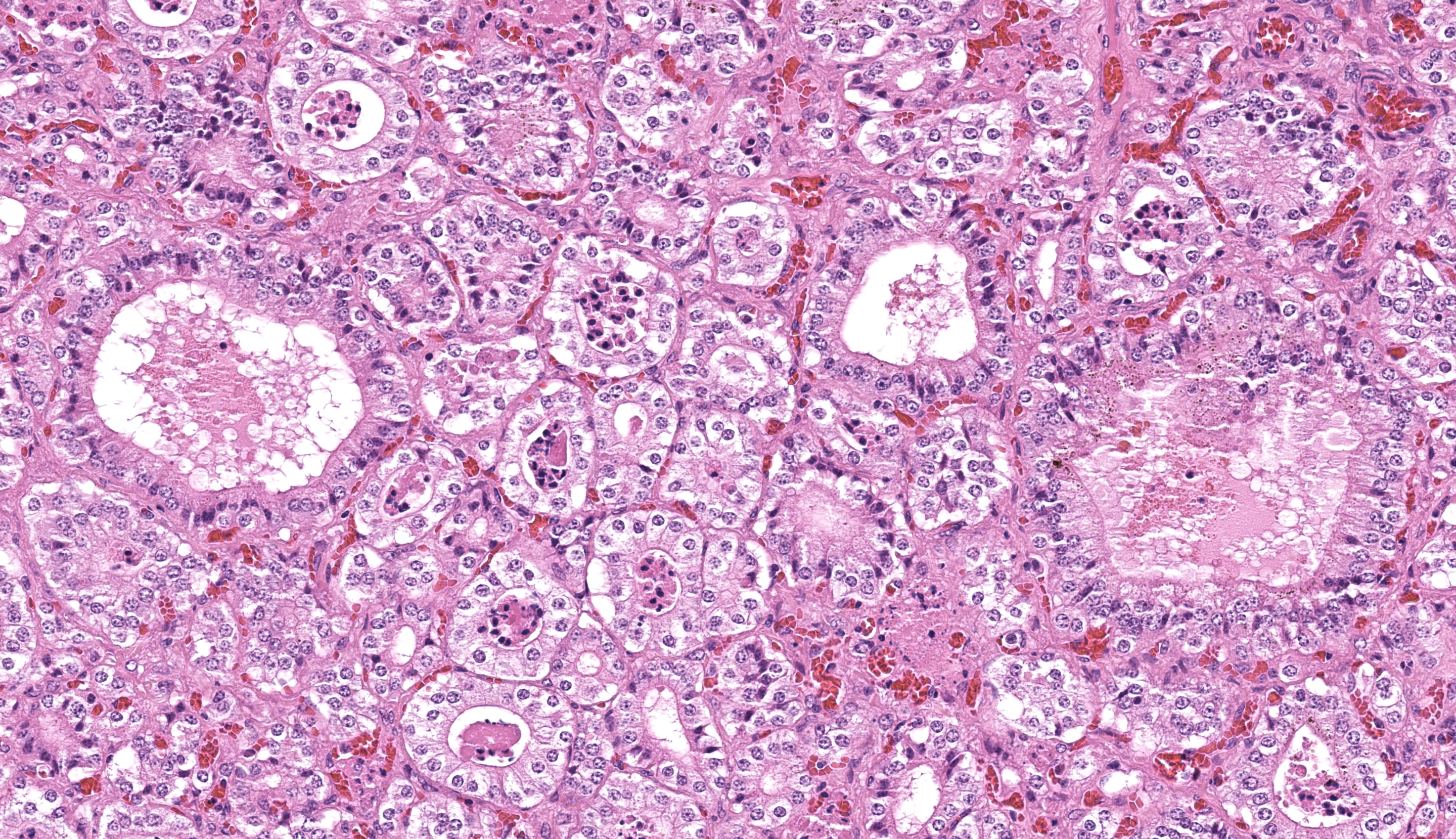
About 20% of follicles have colloid in the lumen and even those had a small diameter. The majority of follicles have no colloid or lumens. The thyroid follicular cells are tall cuboidal to columnar with abundant cytoplasm. Thyroid medullary cells are inapparent.Contributor's Morphologic Diagnoses:
Thyroid follicular cell hypertrophy and hyperplasia, with minimal colloid.Contributor's Comment:
This foal has the macroscopic and microscopic changes of the syndrome of horses known as thyroid hyperplasia and musculoskeletal deformities (TH-MSD) or congenital hypothyroidism-dysmaturity syndrome. Foals with or without musculoskeletal deformities may have microscopic thyroid hyperplasia yet no clinically visible goiter. A variety of musculoskeletal deformities occur.Affected horses are newborn or are aborted. Foals have microscopic hyperplasia of the thyroid gland and may have multiple congenital musculoskeletal deformities. The thyroid gland are usually of normal size macroscopically.
Musculoskeletal lesions include mandibular prognathia, inappropriately ossified carpal and tarsal bones, flexural deformities of the forelimbs and ruptured tendons of the common digital extensor muscles. Foals have either normal or lengthened gestation, and they show signs of immaturity including a short soft coat and lax joints. Aborted foals may have osteopetrosis. It is attributed to micronutrient deficiency including iodine deficiency of the mare. Cases were initially reported in Western Canada but have been found in a variety of other locations in Canada and internationally including Europe. Unless the thyroid gland is examined histologically, the diagnosis will be missed.
Contributing Institution:
Department of Pathobiology, Ontario Veterinary College, University of GuelphJPC Diagnoses:
Thyroid gland: Follicular hyperplasia,diffuse, marked.JPC Comment:
And they're off! This conference is breaking out of the starting gate of the 2025-2026 Wednesday Slide Conference with an equine-centric lineup moderated by the Director of the Joint Pathology Center, COL Sherri Daye. This first case stimulated excellent discussion of a syndrome that is making its debut appearance in the WSC. There have been some great cases of goiter over the years (most recently, WSC 2017-2018, Conf 19, Case 4), but never an equine thyroid hyperplasia and musculoskeletal dysmaturity syndrome (THMSD). Many thanks to the contributor for this unique case. Conference discussion was based largely around the pathogenesis of this condition and potential causes of iodine imbalance in pregnant mares, including consumption of too much or too little iodine or the ingestion of goitrogenic plants (Brassica spp, clover, soybeans, sorghum, etc.). The lack of thyroid C-cells in this condition provided a good exercise for participants in evaluating what is not present and how that is often just as important as seeing what is.Equine THMSD was first described in 1981 in Western Canada when seven foals were submitted to the Western College of Veterinary Medicine for numerous musculoskeletal deformities, where it was determined that all foals also had evident goiter. Since these cases were reported, this syndrome has been described in thousands of foals across Canada, Europe, and the United States. As the contributor stated, many of the foals affected by this syndrome have grossly normal thyroid glands and a range of congenital deformities of variable severity, but all have had histologic evidence of thyroid hyperplasia. Although no exact cause has been decided on, the most widely accepted risk factors include nutritional iodine deficiency and/or high dietary nitrate in the dam leading to the congenital changes in the fetus. In humans, low selenium can also contribute to the development of a similar condition4. Ensuring adequate nutrition of the dam throughout pregnancy is the best prevention.
A quick review of thyroid physiology is warranted to understand the proposed pathogenesis of THMSD. The thyroid gland is responsible for several physiologic functions, including metabolism, thermogenesis, gluconeogenesis, cardiovascular support, neuronal development, and musculoskeletal development. Thyroid hormone production starts with the hypothalamus, which produces thyrotropin-releasing hormone (TRH). TRH acts on the anterior pituitary to stimulate release of thyroid-stimulating hormone (TSH), which is the major regulator of thyroid hormone synthesis in the thyroid gland. These three organs make up the hypothalamic-pituitary-thyroid axis, which allows for negative feedback control of thyroid hormone production. When functioning appropriately, the thyroid gland produces thyroxine (T4) and triiodothyronine (T3), with T3 being the bioactive form. Although low levels of T3 are produced directly, most T3 must be converted within the target cell from T4. That's where the iodine comes in, because conversion of T4 to T3 requires iodine! When there is a lack of iodine, there will not enough bioavailable thyroid hormone being produced. In cases of low thyroid hormone levels, TSH will continue to be produced by the anterior pituitary to stimulate the thyroid glands to produce thyroid hormone. This results in hyperplasia of the thyroid gland, which can become severe enough to cause goiter.
How does this tie in to the musculoskeletal deformities? Thyroid hormone is a critical regulator of energy availability and consumption within the musculoskeletal system6. While the hypothalamus has mostly thyroid hormone receptor (TR), TR is the main receptor expressed in the skeleton and mediates T3 action in bone and cartilage7. Chondrocytes and osteoblasts are directly responsive to thyroid hormone and osteoclastic activity is sensitive to changes in thyroid hormone availability. It's not whether osteoclasts are direct target cells of T3 or if the effects on bone resorption are indirect and mediated by primary thyroid hormone actions in other cells7. Via its action on these cells of the skeleton, thyroid hormone works to regulate intramembranous and endochondral ossification, control the rate of linear growth and bone maturation, and ensure appropriate skeletal mineralization. In an absence of thyroid hormone, these processes are delayed, which can result in the variety of dysmaturities seen in THMSD-affected foals._
References:
- Allen AL. Hyperplasia of the thyroid gland and musculoskeletal deformities in two equine abortuses. Can Vet J. 1995;36: 234-236.
- Allen AL, Doige CE, Fretz PB, Townsend HG. Hyperplasia of the thyroid gland and concurrent musculoskeletal deformities in western Canadian foals: reexamination of a previously described syndrome. Can Vet J. 1994; 35: 31-38.
- Allen AL, Townsend HG, Doige CE, Fretz PB. A case-control study of the congenital hypothyroidism and dysmaturity syndrome of foals. Can Vet J. 1996; 37: 349-351; 354-358.
- Chanoine JP. Selenium and thyroid function in infants, children and adolescents. Biofactors. 2003;19(3-4):137-43.
- Koikkalainen K, Knuuttila A, Karikoski N, Syrja P, Hewetson M. Congenital hypothyroidism and dysmaturity syndrome in foals: First reported cases in Europe. Equ Vet Educat. 2014; 26: 181-189.
- Sindoni A, Rodolico C, Pappalardo MA, Portaro S, Benvenga S. Hypothyroid myopathy: A peculiar clinical presentation of thyroid failure. Review of the literature. Rev Endocr Metab Disord. 2016 Dec;17(4):499-519.
- Williams GR, Bassett JHD. Thyroid diseases and bone health. J Endocrinol Invest. 2018 Jan;41(1):99-109.