Wednesday Slide Conference, Conference 9, Case 4
Signalment:
11-year-old, female, rhesus macaque, Macaca mulatta, nonhuman primate
History:
This macaque has a history of seven liveborn infants by vaginal delivery and recently delivered a large, liveborn male infant with a body weight of 590 g the day prior to presenting for poor maternal care, a retained placenta and suspected endometritis. On physical examination, the placenta was necrotic with an associated purulent exudate and was manually removed. Samples were submitted for aerobic and anaerobic culture. Supportive and therapeutic care was provided. One week after presentation, the uterus was enlarged on palpation and peritonitis was observed on ultrasound examination. She was referred to surgery for exploratory laparotomy. Peritonitis and multiple uterine ruptures were observed. A hysterectomy was performed.
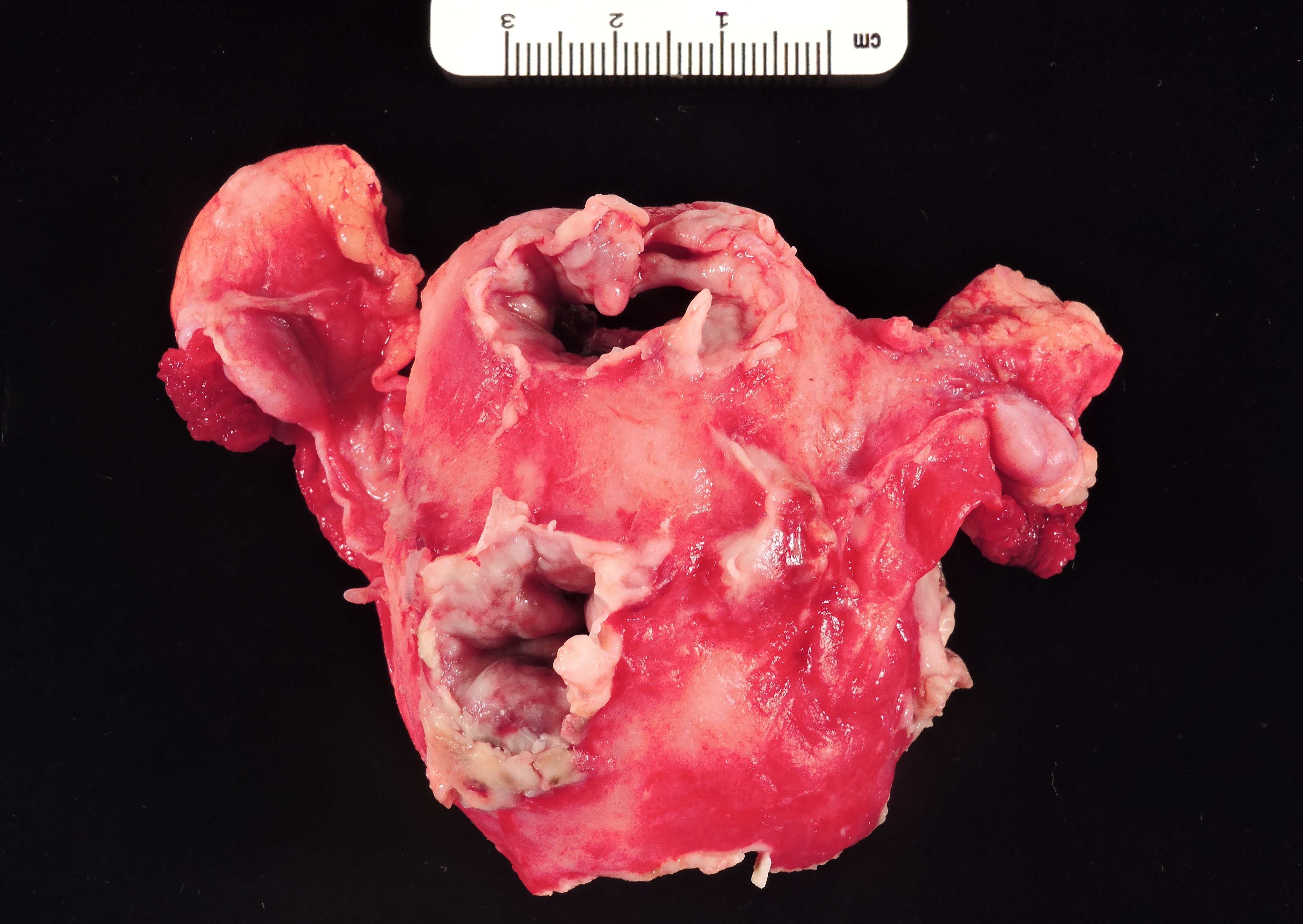
Gross Pathology:
The uterus is enlarged and the integrity of the uterine fundus and the dorsal aspect of the uterine body is disrupted by three transmural, necrotizing uterine ruptures with ragged margins and a fibrinopurulent exudate.
The placental fragments were not submitted for gross or microscopic examination
Laboratory Results:
Aerobic culture of placental fragments yielded a mixed bacterial population at initial presentation - beta-hemolytic Streptococcus (3+), alpha-hemolytic Streptococcus (not Streptococcus pneumoniae, 2+), Proteus (1+), Staphylococcus aureus (1+), and Staphylococcus epidermidis (1+)
Anaerobic culture of placental fragments at initial presentation yielded gram-positive bacillus (not Listeria, 2+), gram-negative bacillus (2+), and gram-positive coccus (3+)
Cytologic examination of the peritoneal fluid one week following initial presentation showed gram-negative bacilli within macrophages and neutrophils.
Aerobic culture of the peritoneal cavity one week after initial presentation yielded Streptococcus, nonhemolytic (4+)
Anaerobic culture of the peritoneal cavity one week after initial presentation yielded gram-positive coccus (3+), gram-negative bacillus (3+) and gram-positive bacillus (1+)
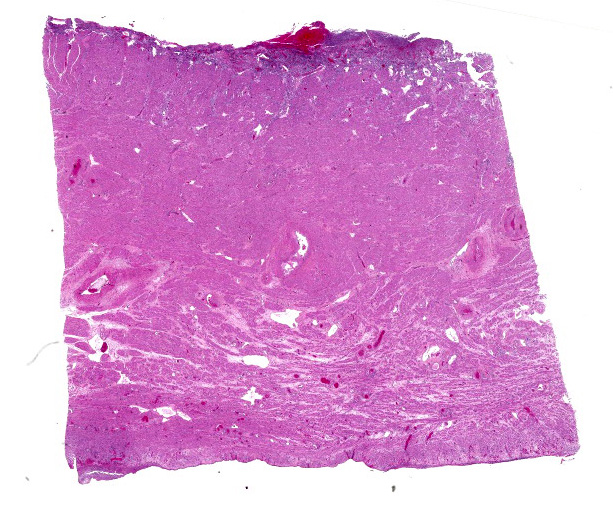
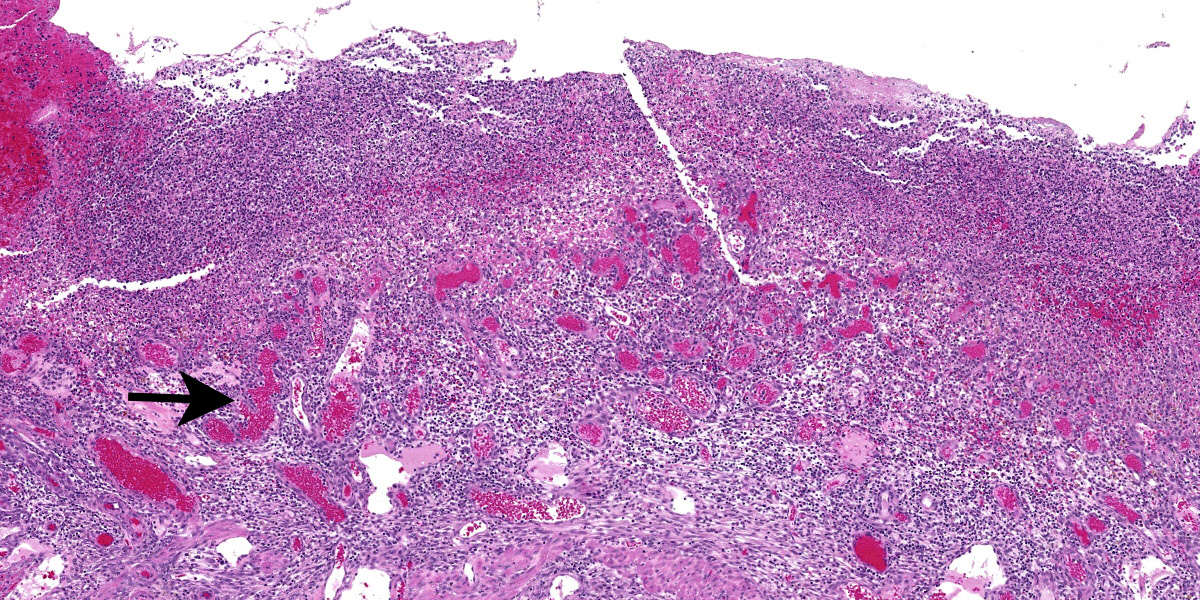
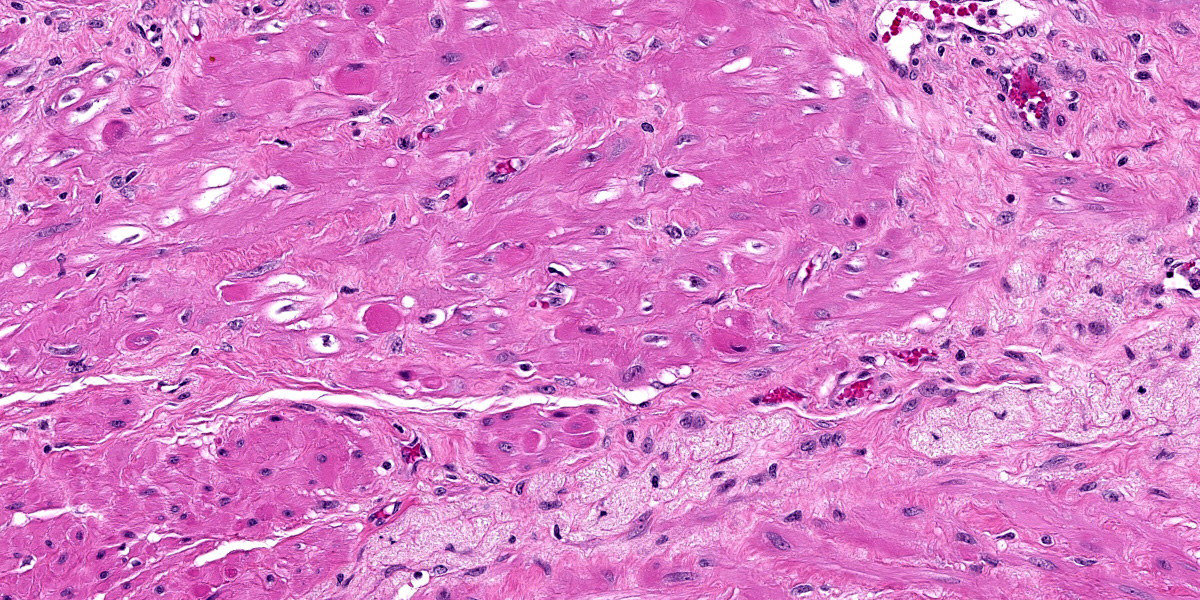
Microscopic Description:
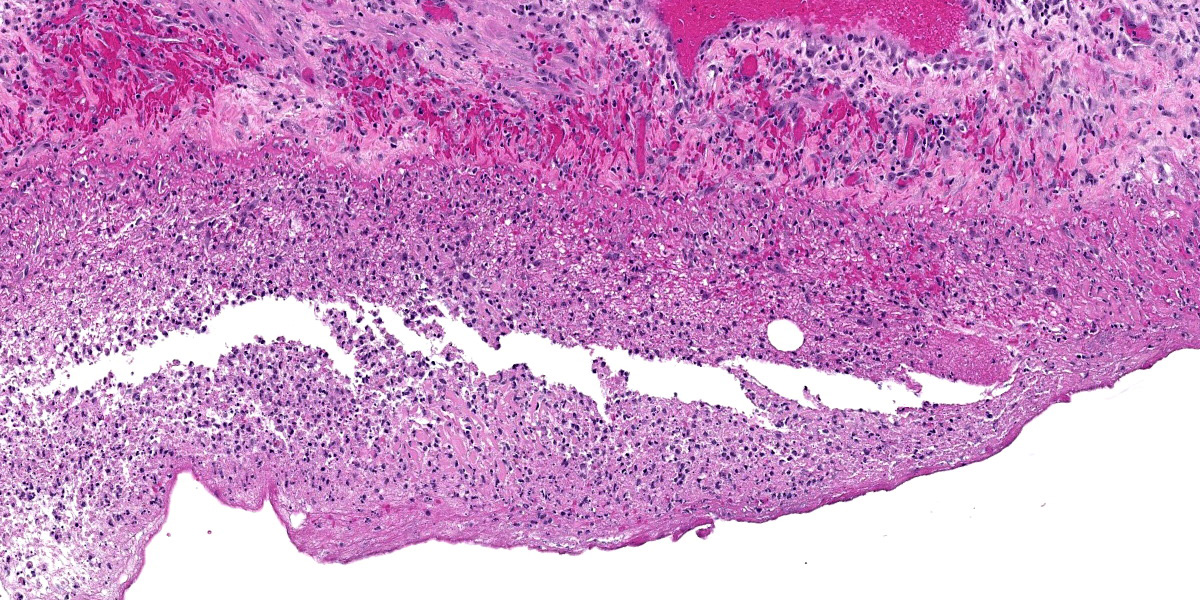
The microarchitecture of the endometrium exhibiting variable stromal decidualization is effaced and overlain by an inflammatory infiltrate composed of myriad degenerate neutrophils, macrophages often laden with brown pigment and fewer lymphocytes admixed with karyorrhectic cellular debris, fibrin, hemorrhage and edema. Endothelial hypertrophy is prominent and there is diffuse congestion. Rare intravascular fibrin thrombi are present. The myofibers of the myometrium immediately subjacent to the endometrium exhibit multifocal, single cell necrosis and multifocally throughout the myometrium there is increased vacuolation of the myofibers. The myometrial interstitium is moderately expanded by fibrous connective tissue and an inflammatory infiltrate composed largely of lymphocytes and plasma cells with few neutrophils surrounds the vasculature. Foci of trophoblastic transformation are present multifocally in the myometrium. The serosa is expanded by degenerate neutrophils, macrophages, fibrin, hemorrhage and karyorrhectic cellular debris. A mixed bacterial population is present within the endometrium and the serosa.
Contributor’s Morphologic Diagnosis:
Uterus: Endometritis, necrotizing, fibrinous, exudative, neutrophilic, histiocytic, lymphocytic, chronic-active, diffuse, severe with serositis, rhesus macaque, Macaca mulatta, nonhuman primate.
Myometrium: Vacuolation, myofibers, generally midsection of the uterus, multifocally extensive, moderate with mild perivascular lymphocytic and plasmacytic infiltrates and moderate interstitial fibrosis.
Oviduct (tissue not submitted): Mesosalpingitis, necrotizing, fibrinous, exudative, neutrophilic, histiocytic, lymphocytic, chronic-active, multifocal, moderate.
Contributor’s Comment:
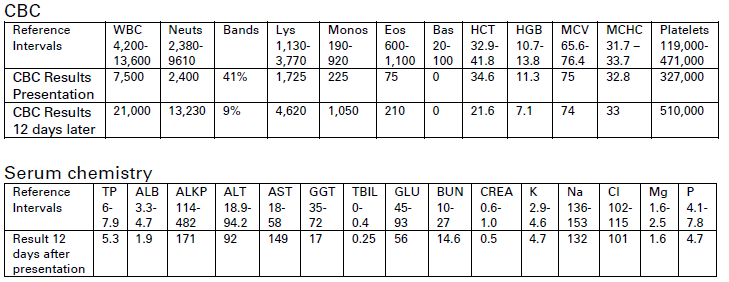
Placental retention, an obstetrical complication may occur with uterine atony or with the placenta accreta spectrum characterized by abnormal adherence of the placenta to the placental bed of the uterus.11 Both entities result in impaired separation and thus release of the placenta. Cervical closure prior to the expulsion of the placenta also results in retained placenta.11 Clinically, the cervix was open in this case. Placenta accreta, increta or percreta may lead to uterine rupture and were not observed on microscopic examination of the submitted tissues. There was no history of uterine trauma or cesarean section that would increase the risk of uterine rupture. In addition to the chronic-active inflammation, this macaque also had moderate interstitial fibrosis in the myometrium and vacuolation of myofibers which may have hampered effective contractions in expelling the infant and placenta. A retained placenta and uterine rupture with resulting hemorrhage would account for the laboratory findings of a normocytic, normochromic anemia and hypoproteinemia and hypoalbuminemia noted 12 days after clinical presentation. The inflammation present in the uterus and abdominal cavity most likely contributed to the depressed albumin levels as albumin is a negative acute phase reactant and also accounted for the remarkable degenerative left shift of 41% in the leukogram at presentation. The pathogenesis in this case of placental retention, endometritis and multiple uterine ruptures followed by peritonitis was considered to be a prolonged, difficult labor involving a large infant, consequent placental retention due to inadequate myometrial contractions and a subsequent, ascending infection through the vagina and open cervix.6
Retained placenta is not an uncommon finding in the breeding colony of rhesus macaques at the Oregon National Primate Research Center. A brief review of the scientific literature revealed a relatively low number of documented cases in nonhuman primates including baboons (Papio spp.),1 cynomolgus macaques (Macaca fascicularis),1,10 rhesus macaques (Macaca mulatta),1 pigtailed macaques (Macaca nemestrina),12,13 a bonobo (Pan paniscus),7 a golden lion tamarin (Leontopithecus rosalia)4 and a chimpanzee (Pan troglodytes).5 Retained placentas in humans range from 1 – 3% of vaginal deliveries.11
Contributing Institution:
Pathology Services Unit
Division of Animal Resources and Research Support
Oregon National Primate Research Center
505 NW 185th Avenue
Beaverton, OR 97006
https://www.ohsu.edu/onprc
JPC Diagnosis:
Uterus: Endometritis, necrohemorrhagic and suppurative, diffuse, marked with endometrial decidual change, multifocal myometrial degeneration necrosis, and fibrinosuppurative serositis.
JPC Comment:
The final case of this conference provided a challenge as tissue identification was not immediately obvious, though the large amount of irregularly arranged smooth muscle was a helpful feature for recognizing the uterus.
Likewise, participants were not aware of the history of this animal before conference, and considered whether the presence of small-caliber blood vessels and loose endometrial stroma could be evidence of granulation tissue secondary to endometritis. In fact, this was actually retained decidua, representing a transient but important part of the maternal uterine connection to the developing fetus and placenta. Similar to granulation tissue, the decidua is modified endometrium composed of large stromal cells and new blood vessels.6 The decidua is formed as part of the menstrual cycle and persists with the establishment of pregnancy. Following parturition, the decidua is shed with the placenta, typically within 24 hours.6 In normal uterine involution, this is represented histologically as regional foci of hemorrhage, inflammatory cells, and necrosis. In this animal however, the placenta was not immediately shed and the degree of inflammation and hemorrhage within the endometrium is entirely in excess. Some participants also noted endometrial spiral arteries in long section which should have also regressed post-partum as another indication of placental retention in this case. Participants did not feel confident that they recognized trophoblasts or syncytial trophoblasts amid the large amount of necrotic debris or embedded deeper within the uterine wall, however.
The degree of uterine myometrial degeneration and fibrosis may represent the cause of uterine rupture in this case. The history of difficult delivery in this animal may be correlated to decreased contractility and ability to expel a large fetus, with the resulting increase in uterine pressure from labor stretching this tissue even further and weakening it. Conference participants surmised that seven previous deliveries may have contributed to these myometrial changes, but that the retained placenta per se was not the initiating cause. The changes in this case were probably consistent with a placental accreta which is defined by an abnormally strong connection to the endometrium by trophoblasts. In contrast, placental increta represent invasion of trophoblasts into the myometrium with placental percreta extending through the uterus entirely and attaching to other viscera such as the urinary bladder.
Finally, this conference concluded with a discussion of resources for considering placental pathology given the large variation between species and even among non-human primates. We have listed these in the references2,3,8 as a courtesy for our readers.
References:
- Bauer C and Harrison T. Retrospective Analysis of the Incidence of Retained Placenta in 3 Large Colonies of NHP. Comp Med. 2016; 66(2):143–149.
- Benirschke, Kurt. Comparative Placentation. UC San Diego. 2012.
- Bowen R. Placental Structure and Classification. Colorado State University. 2011.
- Bronson E, Deem SL, Sanchez C, Murray S. Placental Retention in a Golden Lion Tamarin (Leontopithecus rosalia). J. Zoo Wildl. Med. 2005;36(4):716-718.
- Calle PP and Stringfellow C. Clinical Challenge: Case 2. J. Zoo Wildl. Med. 1991; 22(1):143-145.
- Cline JM, Brignolo L, Ford EW. Urogenital System/Genital System Female/Placental Disorders. In: Abee CR, Mansfield K, Tardif S, Morris T, eds. Nonhuman Primates in Biomedical Research: Diseases. 2nd ed. New York, NY: Elsevier: 2012;522 and 532-533.
- Halbwax M, Mahamba CR, Ngalula AM, Andre C. Placental retention in a bonobo (Pan paniscus). J Med Primatol. 2009;38:171-174.
- Laurent L, Parast M, Mestan K .Comparative Placentation. UC San Diego. 2024.
- Mori M, Bogdan A, Balassa T, Csabai T, Szekeres-Bartho J. The decidua-the maternal bed embracing the embryo-maintains the pregnancy. Semin Immunopathol. 2016 Nov;38(6):635-649.
- Naiken S, Griffiths MA, Edouard L, Padayatchy N. Factors Influencing Reproduction in Captive-Bred Cynomolgus Monkeys (Macaca fascicularis) From Mauritius. Am. J. Primatol. 2015;77:1290–1298.
- Perlman NC and Carusi DA. Retained placenta after vaginal delivery: risk factors and management. Int. J. Women's Health. 2019;11:527-534.
- Ruch TC. Diseases of the Endocrine, Reproductive and Urinary Systems/Reproductive System. In: Ruch TC ed. Disease of Laboratory Primates. Philadelphia, PA: W.B. Saunders Company: 1959;457.
- Stockinger DE, Torrence AE, Hukkanen RR, Vogel KW, Hotchkiss CE, Ha JC. Risk Factors for Dystocia in Pigtailed Macaques (Macaca nemestrina). Comp Med. 2011;61(2):170-175.