Signalment:
Gross Description:
Histopathologic Description:
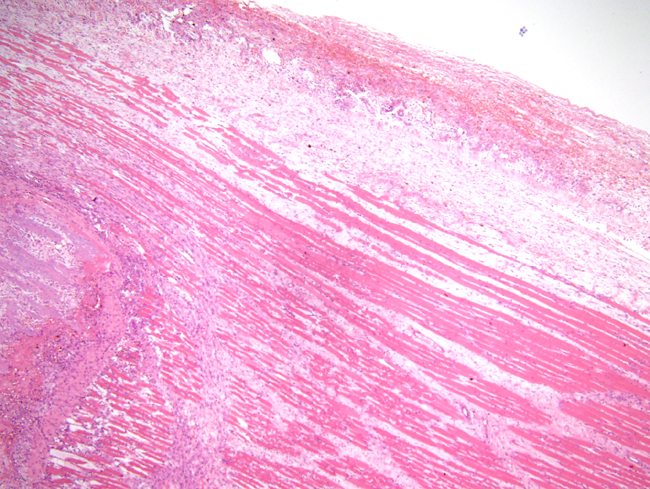
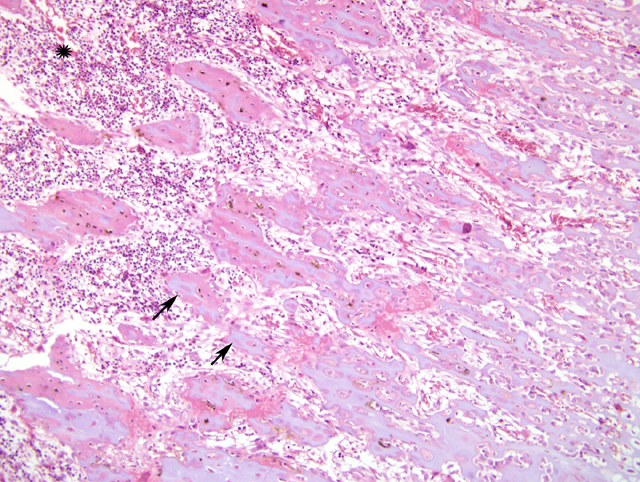
There were no identifiable osteoclasts on the periosteal surface of the diaphysis. The endosteal surface hosted an adequate population of osteoblasts. There was replacement of the terminal plate and cancellous bone of the epiphysis with loose connective tissue containing residual osteoclasts. The growth plate cartilage was disorganised and lacked normal chondrocyte columns. In the primary spongiosa, there was haemorrhage and necrosis, and predominance of spicules that were solely cartilage with no bony transformation. Active resorption of mineralised tissue was occurring and there were fragments of normal spongiosa present, surrounded by loose connective tissue, probably remnants of trabecular fractures. In the tibial metaphysic, there was a well developed scorbutic lattice.
The secondary spongiosa were normal.
Morphologic Diagnosis:
Chronic active haemarthrosis of the stifle joint, with severe chronic active intra-periosteal, intramuscular and periarticular oedema and haemorrhage
Condition:
Contributor Comment:
Vitamin C (ascorbic acid, ascorbate) is water soluble and degraded by heat, ultraviolet radiation or free radical oxidation. Synthesis is widespread in nature, including micro-organisms and fungi. In those vertebrates which synthesise the vitamin, the site(s) of production is in the liver and/or kidneys. Fruit eating bats, red vented bulbul birds, guinea pigs, human and non human primates, most fish and insects lack gulonolactone oxidase to catalyse the last step of the synthesis, and require dietary intake as there is no storage within the body. Absorption occurs in the ileum via active transport.Â
The earliest signs of vitamin C deficiency are generally non specific, such as weakness, anorexia and weight loss. Guinea pigs fed on severely scorbutic diets will voluntarily decrease their intake and begin to lose weight after 2 weeks. After 3 weeks, serum 25OHD3, calcium and albumin levels are significantly reduced, bone mineral density and bone content are significantly lower than normal, and bone volume is reduced in long bones, with fewer and thinner trabeculae and a thinner growth plate. There is also bone loss with osteonecrosis, osteopenia and cortical thinning with periosteal proliferation.Â
The first histological signs in bone are flattening of osteoblasts and failure to lay down matrix. A lattice of vascularised, calcified cartilage is formed in the metaphysis and is not replaced by bone as it increases in thickness; vitamin C is required for the differentiation of osteoblasts from progenitors. Being relatively unresistant to mechanical forces, this scorbutic lattice develops numerous microfractures. Blood vessels of all bone regions dilate, with those of the metaphysis being particularly prominent. Active growth zones are severely hyperaemic and microhaemorrhages are common. Intercellular junctions between endothelial cells are wider in scorbutic vessels than those of normal animals.Â
With time, haematopoietic tissue of the marrow is replaced by immature collagen-poor mesenchyme. In moderately advanced disease, vascularity of the bone is not a prominent feature but vascular fragility is increased. Chondrocyte columns of the growth plate become distorted and shortened as the disease progresses, the number of chondrocytes decreases and the growth plate becomes thin and uneven. Proliferation of spindle cells between the fibrous periosteum and the cortical bone surface thickens the periosteum of long bones, and metaphyseal infarction may occur.
Arthralgia and myalgia develop; eventually bleeding occurs into the joints due to damage to synovial vessels and microfracture of bone. Haemorrhage into stifle joints is among the most obvious signs of scurvy in guinea pigs. There may also be non-haemorrhagic joint effusions. Hair loss and corkscrew hairs are reported; Vitmain C is important in the disulfide bonding of hair. Also reported are follicular hyperkeratosis, and pigmented ichthyosis, fibrosis of dental pulp, diarrhoea and reproductive failure. Wound healing is delayed and incomplete. Conjunctival and intraocular bleeding are also common, and there is disruption of corneal epithelial and stromal organisation with stromal vascularisation in later stages.Â
Laboratory findings are nonspecific. Anaemia is due less to bleeding than to the concomitant iron and folate deficiencies. Foods high in Vitamin C are also sources of folate and the deficiencies often coexist. Furthermore, Vitamin C increases the absorption of nonhaeme iron by reducing ferric iron in the stomach and enhances the amount of iron stored in ferritin. Guinea pigs with lowered levels of vitamin C but normal growth (phase 1 of scurvy) may have serum iron levels decreased to 50% of normal, and by the time clinical scurvy (phase 2) is evident, levels may be as low as 10 15% of normal. Intravascular haemolysis may also lower red cell counts. Leukopenia and hypoalbuminaemia, a marker of malnutrition, are also common.Â
Response to treatment is rapid with most clinical signs reversed within a week of onset of adequate intake. In severely scorbutic guinea pigs, complete restoration of normal trabecular structure takes about 20 to 25 days.
Vitamin C is a major antioxidant, in co-operation with vitamin E and glutathione, and glutathione adminstration can delay the onset of clinical scurvy in guinea pigs. Persistant deficiency leads to hepatocyte apoptosis through endoplasmic reticulum stress as a result of its participation in oxidative protein folding. Oxidative injury in the absence of adequate vitamin has also been linked to motor neuron disease, demyelination of pyramidal tracts and consequent muscular atrophy.
Vitamin C is also an electron donor. It interacts with proline oxidase and lysine oxidase in the hydroxylation of procollagen, in two hydroxylation steps in the production of carnitine, which promotes transport of long chain fatty acids into mitochondria and assists the flux of substrates into the TCA cycle, and with β -monoxygenase in the conversion of dopamine to noradrenaline.Â
The interactions leading to scurvy are not entirely understood. Collagen related signs were thought to be due to failure of hydroxylation of pro-collagen proline and lysine with consequent failure of crosslinking, leading to fibril instability. However, starved animals with vitamin C supplementation show the same reduction in collagen production as scorbutic animals as a result of inhibition of insulin like growth factor (IGF) by binding protein (IGFBP) induction, and deficiency of collagen type IV and elastin leads to defects in blood vessels with consequent haemorrhage in both scorbutic and vitamin supplemented starved animals. Similar effects of IGFBP on collagen are seen in bone, but the decreases in alkaline phosphatase activity are independent of the fasting effect. In cartilage, type II collagen production drops in the early stages of deficiency, but stabilises to around 50% of normal.
The poor wound healing of scorbutic animals, however, is not due to inhibition of proline hydroxylation or induction of IGFBPs. Vitamin C is known to promote wound healing following irradiation through stimulation of collagen synthesis and deposition, and increased fibroblast density and tissue vascularity. Poor wound healing in scurvy may therefore be a consequence of failure of interstitial procollagen gene expression and blood vessel formation.
JPC Diagnosis:
Conference Comment:
Other functions of ascorbic acid include catabolism of cholesterol to bile acids, actions as an antioxidant, folate acid metabolism, and iron absorption.3 In addition to skin, vascular, and skeletal lesions, clinical signs and lesions may include anemia, weakness, myalgia, and myocardial necrosis.3 Common gross skeletal lesions of scurvy include bowing of long bones, outward projection of the ends of the ribs (scorbutic rosary), subperiosteal hematomas, loosening of teeth, and epiphyseal fractures.
The most characteristic histologic feature of scurvy is naked spicules of calcified cartilage, derived from the zone of provisional calcification in the growth plate, that persists as a scorbutic lattice.5 This lattice is particularly susceptible to mechanical stresses and commonly presents with microfractures or infractions with little evidence of normal repair.5
References:
2. Mahmoodian F, Peterkofsky B: Vitamin C deficiency in Guinea pigs differentially affects the expression of type IV collagen, laminin, and elastin in blood vessels. J Nutr 129:83-91, 1999
3. Olmedo JM, Yiannias JA, Windgassen EB, Gornet MK: Scurvy: A disease almost forgotten. Int J Dermatol 45:909-913, 2006
4. Padayatty SJ, Levine M: New insights into the physiology and pharmacology of vitamin C. CMAJ 164:353-355, 2001
5. Thompson K: Bones and joints. In: Jubb, Kennedy, and Palmers Pathology of Domestic Animals, ed. Maxie MG, 5th ed., vol. 1, pp. 136-145. Elsevier Limited, St. Louis, MO, 2007