CASE I: B-14-0576 (JPC 4066399).
Signalment: 9-year-old spayed female Old English sheepdog
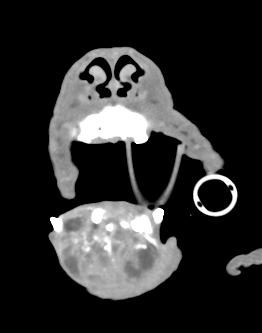
History: The dog had a one-month history of rostral mandibular swelling displacing mandibular incisors and canine teeth. A previous incisional (Jamshidi) biopsy diagnosis was osteosarcoma. A computed tomography scan showed a soft tissue attenuating mass with pinpoint mineral attenuating foci and heterogeneous contrast enhancement; the mass was markedly displacing teeth and causing marked bony lysis and mild osseous proliferation of the rostral mandible (Fig. 1). The mass and rostral mandible including the tissues rostral to teeth 309 and 409 were removed via mandibulectomy and submitted as a surgical biopsy.
Gross Pathology: The mandible contained a smooth surfaced mass covered in mucosal epithelium, which extended from just caudal to the canine teeth to rostral to the incisors, expanding tissue between teeth and widely separating the incisors. The mass measured 4.8 x 4.8 x 3.7 cm, and was firm but not hard and lacked bony texture. On midline section the mass was white to red to dark red, with multifocal cavitated areas filled with watery brown fluid. The interior of the mass was soft with no bony texture.
Laboratory results: NA.
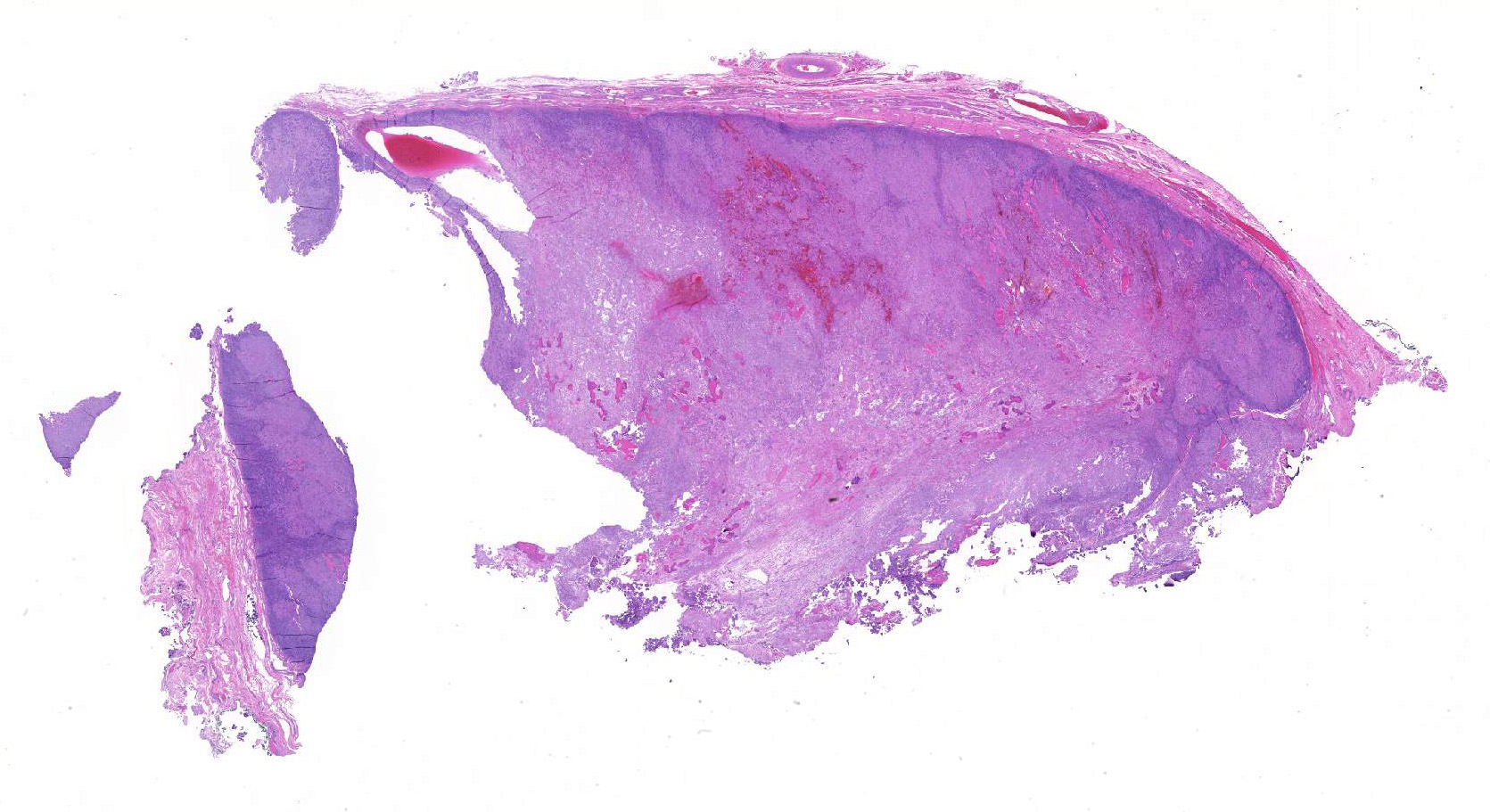
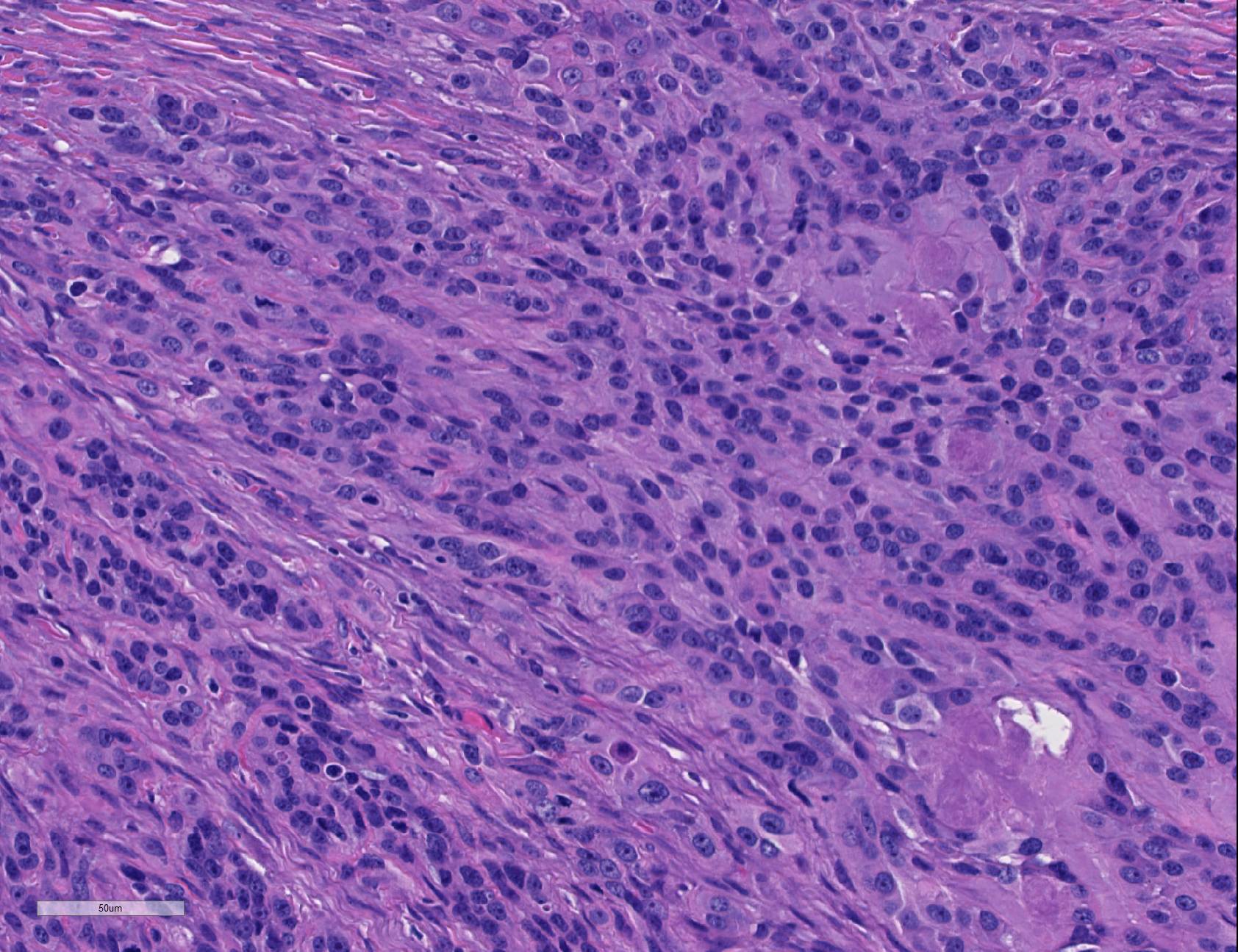
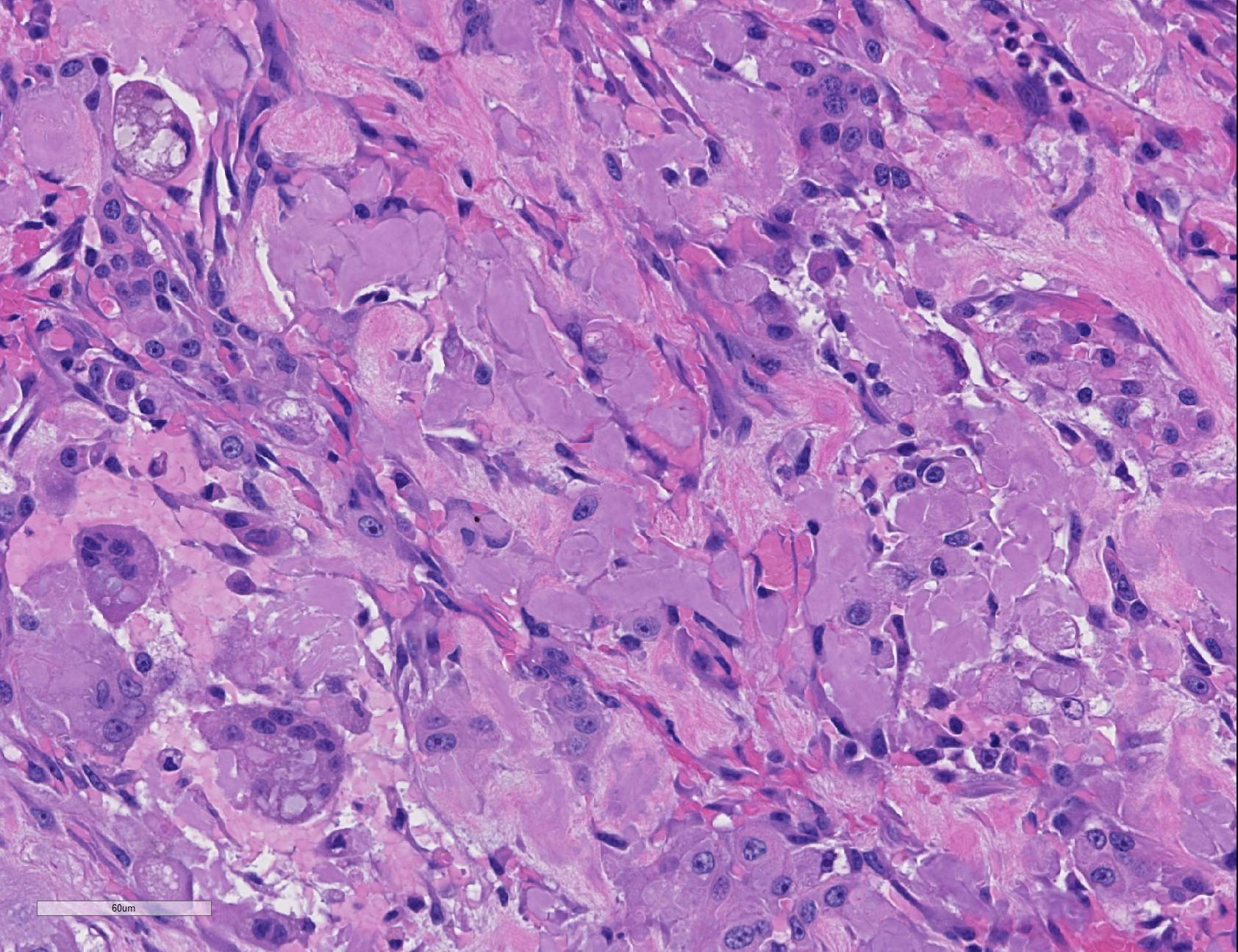
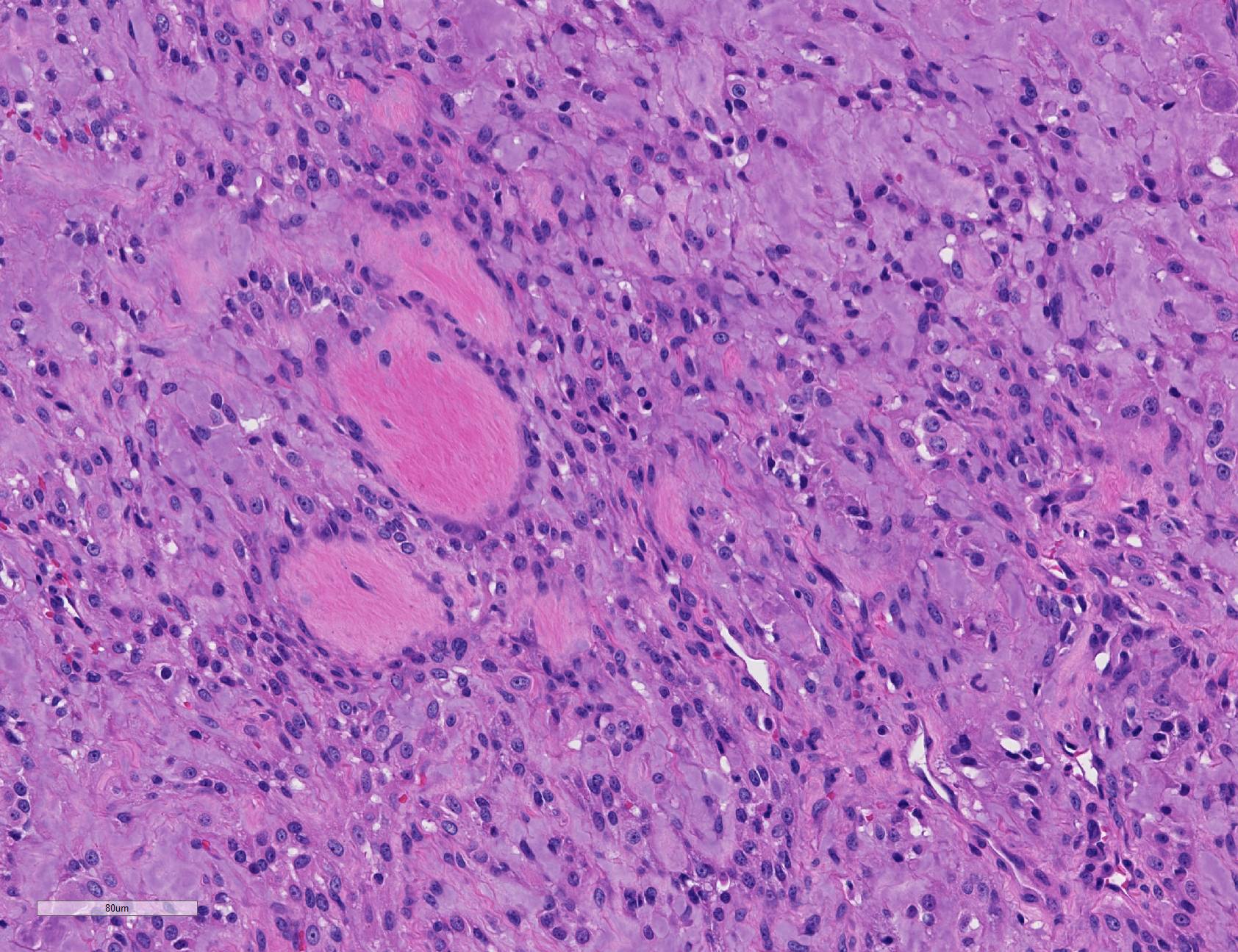
Microscopic Description: The mandible contains and is effaced by an unencapsulated, well-demarcated, multilobulated mass which is composed of polygonal cells arranged in cords, trabeculae, and few small islands, supported by moderate amounts of fibrovascular stroma and with large amounts of extracellular amyloid. The cells are most dense near the edge of the mass, with increasing amounts of matrix centrally, with some central areas showing fewer neoplastic cells and increased amounts of fibrous connective tissue, or cavities of hemorrhage. The cells have distinct borders with rare prominent intercellular bridges, moderate amounts of eosinophilic cytoplasm, oval nuclei with finely stippled chromatin and 1-2 prominent magenta nucleoli. Anisocytosis and anisokaryosis are moderate. Few binucleate and rare multinucleate cells are noted. Mitotic figures are 2 per ten 400x fields. Many cells contain small to large amounts of amphophilic smudgy amorphous material (intracellular amyloid). In some areas cells are larger with more abundant eosinophilic cytoplasm, which occasionally forms concentric lamellae around the nucleus (keratin).
In many areas, cells are separated by moderate to large amounts of extracellular eosinophilic to amphophilic, smudgy, amorphous material (amyloid). In few areas, the cells are separated by islands and trabeculae of densely fibrillar eosinophilic matrix which has a less basophilic tincture than the amyloid and is often mineralized. There are multifocal areas of hemorrhage or necrosis, with few large cavities filled with hemorrhage. Centrally there are regions of loose immature fibrous connective tissue containing few islands of neoplastic cells and matrix. Multifocally the mass is surrounded by a band of moderately cellular collagenous connective tissue with evenly spaced stellate cells reminiscent of periodontal ligament; multifocally these regions have many congested blood vessels and few regular trabeculae of woven bone.
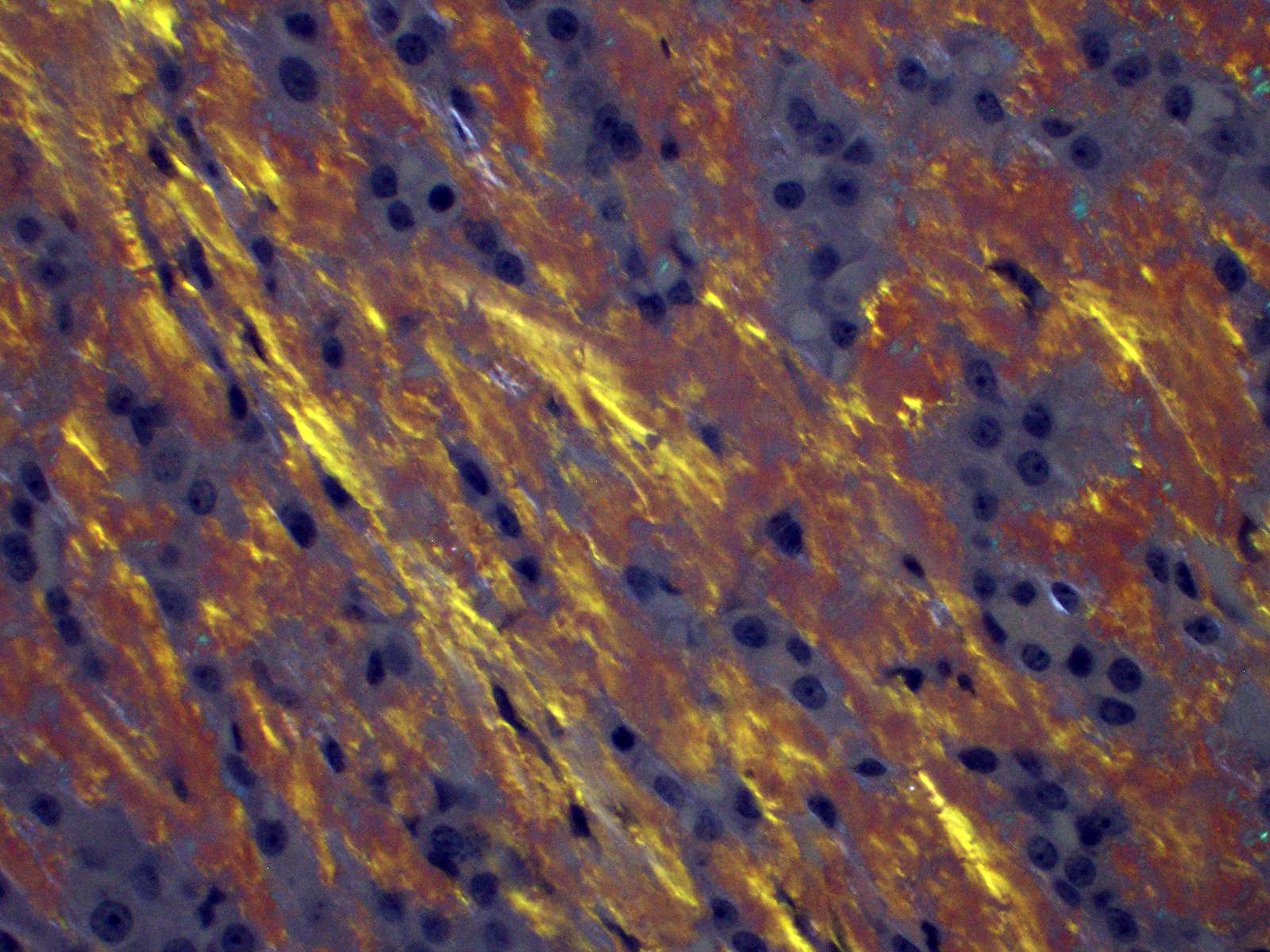
A Congo Red histochemical stain stains the amyloid red, and under polarized light this material has a faint green birefringence.
Pancyokeratin (AE1/AE3) and vimentin immunohistochemistry both show strongly positive cytoplasmic labeling in neoplastic cells. The amyloid is weakly immunopositive for pancytokeratin.
Contributor Morphologic Diagnosis:
Rostral mandible: amyloid-producing odontogenic tumor
Contributor Comment: Amyloid-producing odontogenic tumor (APOT) is a rare neoplasm reported in dogs and cats.1 Histologically they are characterized by odontogenic epithelium with extracellular and intracellular congophilic amyloid matrix. Features of odontogenic epithelium include thin trabeculae and islands of cells with centrally located cells having long intercellular bridges, and peripheral palisading cells with apical nuclei and basilar cytoplasmic clearing. These classical features may be difficult to demonstrate in some tumors, as in this case. Odontogenic epithelium may co-express both cytokeratin and vimentin,3 as demonstrated in the immunohistochemistry results. Biologic behavior is slowly progressive but metastatic APOT has not been reported. Complete surgical removal is the treatment of choice. The nature of the amyloid protein in this tumor is reported to be a combination of enamel proteins.2 This tumor has also been referred to as ?calcifying epithelial odontogenic tumor?, but the term is borrowed from a human condition with several distinctly different features from APOT, including mineralization of matrix and sheets of polygonal cells.1,4 APOT is not reported in humans.
Contributing Institution:
University of Wisconsin-Madison, School of Veterinary
Medicine, 2015 Linden Drive
Madison, WI 53706
www.vetmed.wisc.edu
JPC Diagnosis: Gingiva: Amyloid-producing ameloblastoma.
JPC Comment: Amyloid-producing odontogenic tumors (APOT), are rare tumors of the oral cavity and have been reported in dogs, cats, and in a goat, horse, rabbit, moose, Bengal tiger and a prairie dog.6,9 These rare tumors have been reported to comprise between 1 and 4% of odontogenic neoplasms in the dog.8 It has also been recently reported in the facial skin of cats within the supraorbital and labial skin.4
This history of this neoplasm has not been without controversy, as evidenced by the many names by which it has been referred to over the years. Originally diagnosed in humans in 1958 by J.J. Pindborg, the neoplasm in many early veterinary texts was referred to as a calcifying epithelial odontogenic tumor (CEOT) or " Pindborg tumor" , but a 1994 publication by Gardner et al provided evidence that the human and veterinary versions of the neoplasm were distinct entities and proposed the name amyloid-producing odontogenic tumor.9 Recent publications have suggested that the CEOT and APOT may be two stages along a spectrum of a tumor which produces a variety of substances such as dental hard substances such as cementum and dentin, amyloid, and keratin9. In a recently published textbook on veterinary oral and maxillofacial pathology, the tumor is referred to as an amyloid-producing ameloblastoma.9
These neoplasms are unencapsulated neoplasm that may arise either centrally or peripherally within the bone, which while widely considered benign, may aggressively invade bone.8,9 The tissue or origin is not clear, and current thought of origin include some component of odontogenic epithelium of the dental lamina, stratum intermedium of the enamel organ, or Hertwig?s epithelial root sheath.9 The appearance of the epithelial component may vary widely from traditional columnar to spindled or even round in less differentiated regions of the tumor.9 Some feline tumors may even have melanin granules within the epithelial component.9 Pancytokeratin and vimentin may be helpful in differentiating between epithelial, stromal, and inflammatory components.
The deposition of amyloid is the defining characteristic of this particular neoplasm. Amyloid within APAs has been shown to be different from AA, AL, and senile cardiovascular amyloid.8 Odontogenic amyloid ameloblast-associated protein (ODAM), a feature of human CEOTs has not been identified within these tumors (supporting their distinction from the human CEOT), a number of other amyloid-related proteins have been found in canine and feline APAs, including amyloid protein of canine APOT, ameloblastin (also present in cat APAs), amelogenin, and sheathlin.4,8 While the amyloid material in this case demonstrates congophilia and green birefringence on polarized light, the material is not always birefringent.9 Some authors believe that the amyloid-like material represents dysplastic tooth matrix, as immunohistochemical analysis of the amyloid protein in several studies has indicated that it is of ameloblastic origin.1, 3
References:
1. Delaney MA, Singh K, Murphy CL, Solomon A, Nel S., Boy SC. Immunohistochemical and biochemical evidence of ameloblastic origin of amyloid-producing odontogenic tumors in cats. Vet Pathol 50(2): 238-242.
2. Head KW et al. Histologic classification of the tumors of the alimentary system in domestic animals. Washington DC, Armed Forces Institute of Pathology CL Davis DVM Foundation, 2003.
3. Hirayama K, Miyasho T, Ohmachi T, Watanabe T, Yokota H, Taniyama H. Biochemical and immunohistochemical characterization of the amyloid in canine amyloid-producing odontogenic tumor. Vet Pathol. 2010;47:915-22.
4. Hirayama,K, Endoh C, Kagawa Y, Ohmachi T, Yamagami T, Nomura K, Matsuida K, Okamotis M. Taniyama H. Amyloid producing odontogenic tumors of the facial skin in three cats. Vet Pathol 2017; 54(2): 218-221.
5. Izzati UZ, Hidaka Y, Hirai T, Yamaguchi R. Immunohistochemical profile of ameloblastic carcinoma arising from an amyloid-producing odontogenic tumor in a miniature dachshund. J Comp Path 2019; 106:54-58.
6. Kok, MK, Chamgers JK, Ushio N, Miwa Y, Nakayhama H, Uchida K. Amyloid-producing odontoameloblastoma in a black-tailed prairie dog. J Comp Path 2018; 159:26-30.
7. Miles CR, Bell CM, Pinkerton ME, Soukup JW. Maxillary ameloblastic fibroma in a dog. Vet Pathol. 2011;48:823-6.
8. Munday JS. Lohr CV, Kiupel M. Tumors of the alimentary tract. In: Meuten DJ, ed., Tumors in Domestic Animals, 5th Ed, Ames IA: Wiley and Sons, 2017: 536-537.
9. Murphy BG, Bell CM, Soukup JW. Tumors composed of odontogenic epithelium and fibrous stroma. In: Veterinary Oral and Maxillofacial Pathology. Hoboken, NJ: Wiley and Sons, 2020, pp. 105-108
10. Regezi JA, Sciubba JJ, Jordan RCK. Odontogenic tumors. In Oral Pathology: Clinical pathologic correlations. St Louis MO Saunders Elsevier, 2008.