WSC 22-23
Conference 14
Case I:
Signalment:
14 years old, female-neutered, domestic shorthair cat, feline, Felis catus
History:
The owner noted a 3 x 4 x 3 cm subcutaneous mass on the left ventral aspect of the mandible and cranial aspect of the neck. On clinical examination, an enlarged mandibular lymph node was diagnosed. The other palpable lymph nodes were normal in size and no other symptoms or lesions were detectable. Laboratory parameters were unremarkable. Serologic tests for FeLV and FIV were negative. The owner opted for surgical removement, and histopathologic examination was initiated.
The postoperative interval was initially unremarkable; there was no evidence of metastasis or recurrence. Three months after surgery, the animal developed deteriorated general condition, inappetence, and vomiting. Multiple cranial lymph nodes were moderately swollen. Radiologically, an intrathoracic mass associated with the trachea was detected, and both kidneys were enlarged. Progression of malignancy was feared. Brief palliative therapy with prednisolone and antibiotics for several days was given. Due to the deteriorating condition, the owner opted for euthanasia. At postmortem examination, multiple lymph nodes on the head and neck were similarly enlarged. A firm white mass 1 x 2 x 1 cm in diameter was noted on the intrathoracic aspect of the trachea. Both kidneys were enlarged and soft, and the cortex was diffusely pale white in color with some hemorrhages.
Histopathologically and immunohistochemically, the enlarged lymph nodes showed the same neoplastic cell population as in the initially removed lymph node, and both kidneys and the tracheal mass showed the same neoplastic infiltration.
Gross Pathology:
A 4.5 x 3.5 x 2 cm firm lymph node was processed, and the cut surfaces were homogeneously yellow-white in color.
Laboratory Results:
|
Marker |
Normal cell type |
T7562/21: multinucleated cells (H-RS cells) |
T7562/21: monomorphic lymphatic cells (bystander cells) |
Other findings |
|
CD3 (polyclonal) |
T cells |
- |
+++ |
Residual perifollicular cells/T cells ++ |
|
CD3 (monoclonal) |
T cells |
- |
+++ |
Residual perifollicular cells/T cells ++ |
|
CD45R (B220) |
Feline B cells |
- |
+ |
Residual cortical lymphoid follicles/B cells ++ |
|
CD20 |
B cells |
- |
- |
No reactivity |
|
Pax-5 |
B cells |
- |
- |
Residual cortical lymphoid follicles/B cells ++ |
|
BLA.36 |
B cells |
+++ |
+++ |
Residual cortical lymphoid follicles/B cells ++ |
|
IBA-1 |
Macrophages, monocytes, histiocytes |
- |
- |
Single dendritic cells + |
|
CD30 |
H-RS cells |
+++ |
- |
No reactivity |
|
CD15 |
H-RS cells |
- |
- |
No reactivity |
|
Ki-67 |
Proliferating cells |
+ |
++ |
30-50 positive nuclei/HPF (0.237 mm2) |
H-RS cells: Hodgkin Reed-Sternberg cells. - negative; + few positive cells; ++ more positive cells; +++abundant positive cells; H-RS cells: Hodkin and Reed-Sternberg cells.
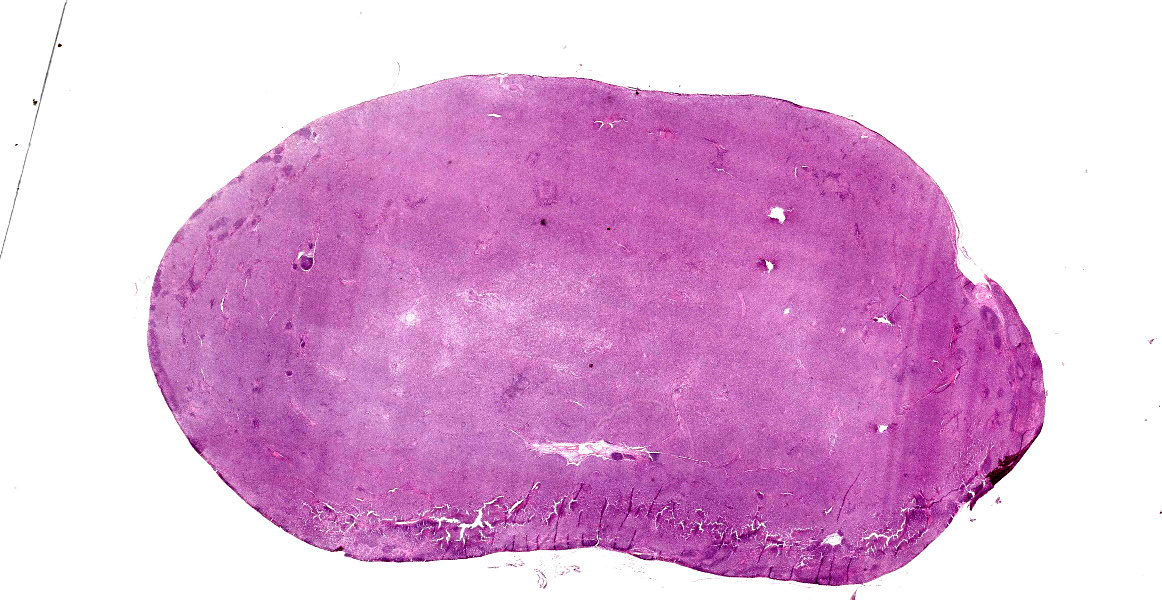
Microscopic Description:
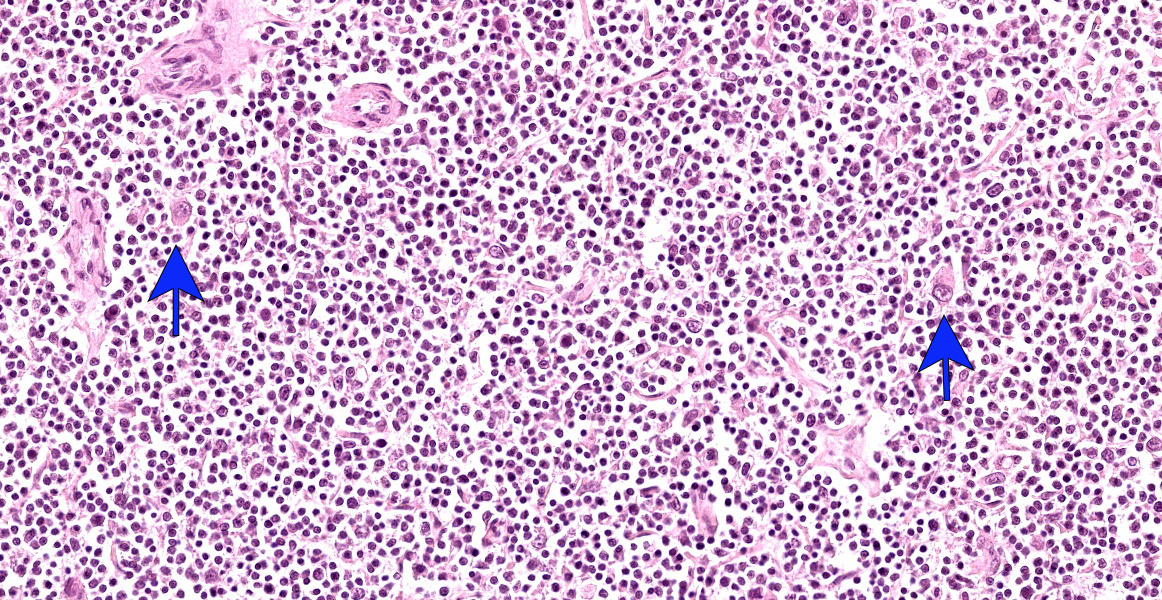
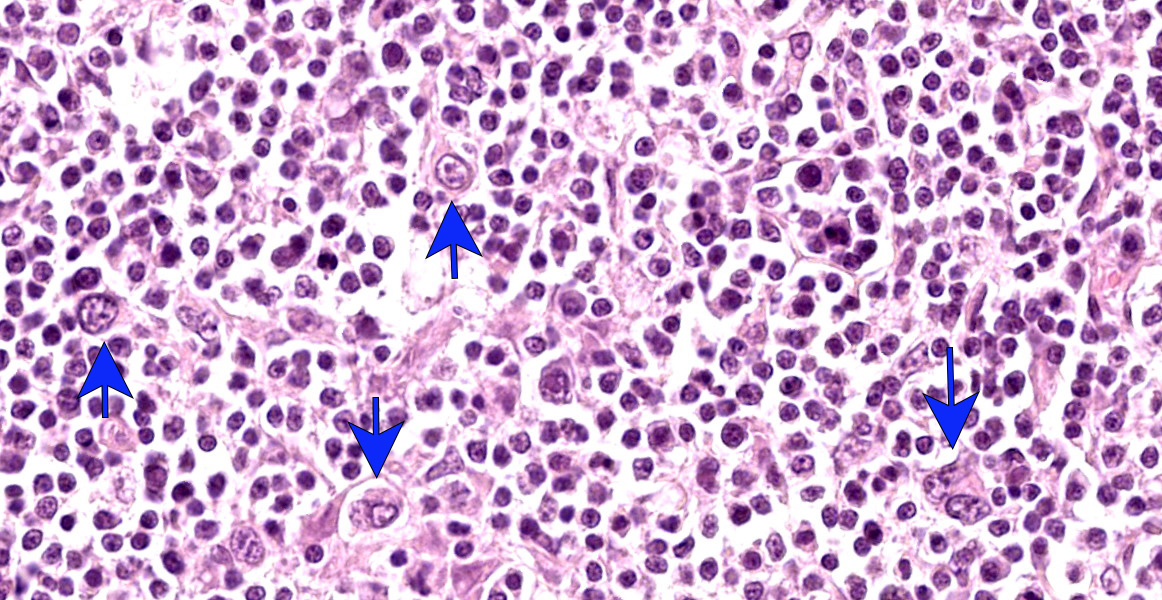
Lymph node: A densely cellular, poorly demarcated, infiltrative, unencapsulated neoplasm composed of moderate numbers of neoplastic cells on a lymphocytic background and a preexisting fibrovascular stroma effaces the lymph node architecture and compresses the remaining follicles. The neoplastic cells are irregularly polygonal and up to 120 micrometer in diameter with distinct cell borders and abundant eosinophilic cytoplasm. The nuclei define two subtypes of neoplastic cells: Hodgkin cells are mononuclear with a single round to oval nucleus. Reed-Sternberg cells have at least two nuclear lobes or nuclei, but can have up to 5 irregular oval to polygonal (multilobulated) nuclei. The chromatin of both cell types is coarsely stippled to clumped, and the nucleoli are variably visible but often multiple. Rarely, the nucleoli are amphophilic and surrounded by a halo. Multifocally, single neoplastic cells have condensed cytoplasm and pyknotic nuclei ("mummified" Hodgkin cells). There is marked anisocytosis and anisokaryosis, and the mitotic count averages 5 mitoses in 10 high-power fields (2.37 mm2). Often the mitoses are bizarre.
Contributor’s Morphologic Diagnoses:
Mandibular lymph node: Hodgkin-like malignant lymphoma, cat, Felis catus
Contributor’s Comment:
Lymphomas account for approximately 80% of all hematopoietic neoplasms in domestic animals, and both categorization and classification have been revised and changed several times in the past. Oncologists use different treatment strategies, and follow-up data are often limited.8,9,10 In addition, diagnoses may vary between pathologists and/or hematopathologists. A still very useful first classification tool is tumor topography. In cats, more than 50% are alimentary forms, whereas in dogs multicentric forms predominate.11
The epidemiology of feline lymphomas has changed dramatically in the past due to the successful vaccination campaign against FeLV.9,10 Previously, approximately 30% of feline neoplasms were malignant lymphomas and 80% of these were associated with FeLV infection.
In animals, most lymphomas resemble human non-Hodgkin lymphomas, but in some species Hodgkin or Hodgkin-like lymphomas have also been described: for example, a well-characterized case in a ferret.5
In 1832, Thomas Hodgkin described a series of seven cases of lymph nodes with unusual changes, now known as Hodgkin lymphoma. In humans, the disease shows a bimodal age distribution with peaks in young adults and the elderly in developed countries. In developing countries, the first peak affects children. Often the disease is localized, with only a few cases being widespread. Overall, this type of lymphoma is considered moderately aggressive but curable in most cases. The typical neoplastic cells are CD30+, usually CD15+, negative for most B-cell markers, typically negative for T-cell markers, negative for immunoglobulin, negative for CD45, and negative for anaplastic lymphoma kinase (ALK). Pax5 is usually expressed by the neoplastic cells.3
In veterinary medicine, Hodgkin-like lymphoma appears to be a predominately feline entity manifestating in the upper respiratory and alimentary tract.7,12 One report described an unusual manifestation of Hodgkin-like lymphoma in the cerebellum of a FeLV-infected cat.13 Cytologically and histopathologically, the presence of scattered large mononucleated and binucleated to multinucleated cells (Hodgkin and Reed-Sternberg cells, HRS cells) should favor the diagnosis of Hodgkin-like lymphoma. However, immunohistochemistry is required for definitive diagnosis. Many cases appear to be misinterpreted as T-cell-rich B-cell lymphomas.9,10
There are some reports of problems with immunohistochemical staining of B cells in cats.10 CD79-alpha staining, which is well reproducible in dogs, often showed variable results in our laboratory in cats (as did occasionally staining with CD20). Therefore, in the last two decades, the B-cell-specific variant of CD45R (B220) has been preferred by us, as well as by some other laboratories, for B cells in cats. Parallel staining with Pax5 showed reproducible results.2
Our case of feline Hodgkin-like lymphoma was well documented clinically, and follow-up examinations including necropsy was performed. Immunohistochemical results (see Table) supported our morphologic diagnosis. The malignant potential in this presented case was obvious.
Contributing Institution:
Institut fuer Veterinaer-Pathologie, Justus-Liebig-Universitaet Giessen
Frankfurter Str. 96, 35392 Giessen, Germany
http://www.uni-giessen.de/cms/fbz/fb10/institute_klinikum/institute/pathologie
JPC Diagnosis:
Lymph node: Lymphoma, large cell, with Hodgkin-like features.
JPC Comment:
Hodgkin lymphoma typically presents as a single enlarged node, or enlargement of multiple contiguous nodes. In humans, these nodes are typically cervical, mediastinal, or para-aortic, and in cats, they are typically mandibular, cervical, or mediastinal.5,7,12 The neoplasm is thought to arise from germinal or post-germinal center B cells. In humans, neoplastic cells commonly contain increased NF- κB activity, either due to infection by Epstein Barr virus (human herpesvirus 4) or decreased activity of NF-κB suppressors such as IκB.5 Neoplastic cells produce various cytokines and chemokines which cause influx of a mixed population of leukocytes (lymphocytes, granulocytes, and macrophages); thus neoplastic cells, which are typically giant with abnormal nuclei, account for less than 5% of the cell population within the tumor.5,12
The classic neoplastic cell in Hodgkin lymphoma is the Reed-Sternberg cell, as the contributor describes. These cells are up to 45 um in diameter and contain bi-lobed nuclei with large nucleoli up to 7 um in diameter, giving the cell an “owl eye” appearance.5,12 Mononuclear, multi-nucleated, and lacunar variants of Reed-Sternberg cells also occur. In lacunar variants, the nuclei are folded and surrounded by cytoplasmic clearing due to processing artifact. Reed-Sternberg cells are the predominant neoplastic cell type in classic Hodgkin lymphomas, which can be divided into at four subtypes: nodular sclerosis, mixed cellularity, lymphocyte-rich, and lymphocyte-depletion.5 These subtypes have similar IHC staining characteristics, but distinct histologic and clinical features.5
Another neoplastic cell type, the lymphohistiocytic variant (L&H cell), is seen in a distinct subtype, the nodular lymphocyte-predominance Hodgkin lymphoma. These cells are also known as “popcorn” cells because of their unique appearance: vesicular, polypoid nuclei with fine chromatin and indistinct nucleoli bear some resemblance to popped popcorn. L&H cells have distinct IHC staining pattern and are generally negative for both CD15 and CD30 and positive for CD20, CD45, and CD79.5,7
A report of 20 cases of Hodgkin-like lymphoma in cats provides some insight into this neoplasm, which is uncommon in cats and rare in other veterinary species.12,14 Unilateral mandibular or cervical lymph node swelling was observed in 18 of 20 cats.12 Eleven of the cats had classic forms, with nine classified as mixed cellularity and two classified as the nodular sclerosis substype.12 Nine cats had the lymphocyte-predmoninant Hodgkin lymphoma, with L&H cells predominately surrounded by non-neoplastic small lymphocytes.12 This study suggested that, as in humans, Hodgkin-like lymphoma is less aggressive than non-Hodgkin lymphoma in cats; however, additional data is needed for statistically significant correlation.12
Cases for this week’s conference were selected to highlight human-animal correlates in medicine. This week’s moderator, Dr. Sarah Cudd, discussed the clinical, pathologic, and historical aspects of the disease in humans. Human MD pathologists at the Joint Pathology center were also consulted on this case, and they favored a diagnosis of malignant B cell lymphoma with Hodgkin-like features, though T-cell/histiocyte-rich large B cell lymphoma could not be ruled out.
References:
- Carminato A, Tecilla M, Roccabianca P, Zanardello C, Melchiotti E, Capello K, Vascellari M. CD30 Cross-Reactivity and Expression in Feline Normal Tissues and Lymphomas. Vet Pathol. 2020; 57: 49-55.
- Felisberto R, Matos J, Alves M, Cabeçadas J, Henriques J. Evaluation of Pax5 expression and comparison with BLA.36 and CD79αcy in feline non-Hodgkin lymphoma. Vet Comp Oncol. 2017;15:1257-1268.
- Ferry JA. Thomas Hodgkin and Hodgkin lymphoma. J Hematopathol. 2014;7:123-138.
- Hodgkin T. On some morbid appearances of the absorbent gland and spleen. Med Chir Trans. 1832;17:69–97.
- Kumar V, Abbas AK, Aster JC, Turner JR. Robbins and Cotran Pathologic Basis of Disease. 10th Philadephia, PA: Elsevier: 2021: 611-616.
- Matsumoto I, Uchida K, Chambers JK, Nibe K, Sato Y, Hamasu T, Nakayama H. Hodgkin's-like lymphoma in a ferret (Mustela putorius furo). J Vet Med Sci. 2017;79:1660-1663.
- Steinberg JD, Keating JH. What is your diagnosis? Cervical mass in a cat. Vet Clin Pathol. 2008;37:323-327.
- Valli VE, Jacobs RM, Parodi AL, Vernau W, Moore PF. Histological classification of tumors of hematopoietic tumors of domestic animals. WHO, Washington, DC: Armed Forces Institute of Pathology; 2002, 2nd Series, vol. 8.
- Valli VEO, Kiupel M, Bienzle D, Wood RD. Hematopoietic system. In: Maxie MG, ed. Jubb, Kennedy, and Palmer’s Pathology of Domestic Animals. Vol 3. 6th ed. Philadelphia, PA: Elsevier; 2016:102-268.
- Valli VE, Bienzle, D, Meuten, DJ: Tumors of the hemolymphatic system. In: Meuten DJ, ed. Tumors in Domestic Animals. 5th ed. Ames, IA: Wiley Blackwell; 2017: 203-321.
- Vezzali E, Parodi AL, Marcato PS, Bettini G. Histopathologic classification of 171 cases of canine and feline non-Hodgkin lymphoma according to the WHO. Vet Comp Oncol. 2010; 8: 38-49.
- Walton RM, Hendrick MJ. Feline Hodgkin's-like lymphoma: 20 cases (1992-1999). Vet Pathol. 2001; 38: 504-511.
- Yoshino Y, Chambers JK, Nakamori T, Goto-Koshino Y, Nishigaki K, Tsujimoto H, Matsuki N, Nakayama H, Uchida K. Primary cerebellar lymphoma with Hodgkin lymphoma-like morphology in a cat. J Vet Diagn Invest. 2017; 29: 707-710.
- Vail DM, Pinkerton M, Young KY. Hematopoietic Tumors. In: Vail DM, Thamm DH, Liptak J, eds. Withrow and MacEwen’s Small Animal Clinical Oncology. 6th ed. Philadelphia, PA: Elsevier. 2019: 715-729.