Signalment:
Gross Description:
Histopathologic Description:
Morphologic Diagnosis:
Condition:
Contributor Comment:
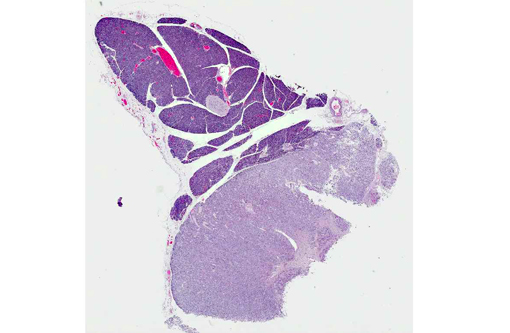
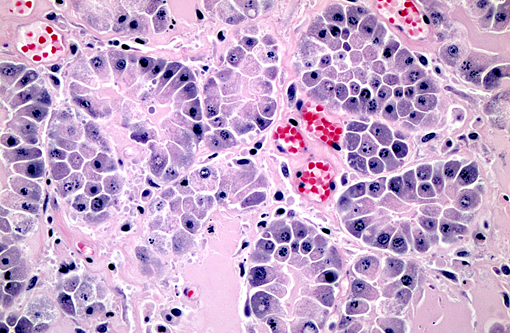
Carcinomas may be manifest as single or multiple masses in the organ. They are histologically variable and are classified as acinar, which look like normal exocrine tissue, tubular, which appear more similar to ducts, or undifferentiated, when cells occur in sheets. Hyalinizing carcinomas contain interstitial glassy eosinophilic matrix in tubular lumina or expanding the matrix.(1) This substance is not congophilic and fails to stain immunohistochemically with reagents to serum amyloid A, amylin, α1-antitrypsin or immunoglobulin light chain. The nature of this matrix is not known. In a small case series, these carcinomas tended to favor the acinar pattern and patients that were not euthanized immediately after surgery had a somewhat longer survival than expected.(1) A case with clear cell morphology and similarly increased interstitial matrix has been recently reported in a dog, in which the matrix was PAS+.4 Our case has a mixed pattern with sheets of undifferentiated cells as well as acini.
Cytokeratin labeling has been disappointing(2) for use in identifying pancreatic carcinomas in dogs, and has the draw-back of staining cytokeratin on other organs when utilized to identify metastases. In cats pancreatic exocrine neoplasms are often positive for one or both reagents, as is normal pancreas. In dogs, pancreatic ducts are reported to express cytokeratin 7, but acini were negative, while acinar tissue reacted with neither reagent. Four pancreatic exocrine neoplasms tested in this series were also uniformly negative. Recently claudin-4 has been suggested as a reagent useful in negative poorly differentiated exocrine tumors and ductular tumors from between differentiated acinar neoplasms, which are positive.(3)
The patient had very severe rear leg swelling with marked subcutaneous edema, which histologically was found to contain numerous neutrophils. Two of the cases in reference 1 also had one or more areas of suppurative panniculitis, although the lesions were in other locations. This patient had severe postcaval compression from one of its hepatocellular carcinomas, and this may have been the cause of edema.
JPC Diagnosis:
Conference Comment:
Canine hyalinizing pancreatic adenocarcinoma is a well-differentiated, solitary mass most commonly seen in the right limb of the pancreas. The most frequent clinicopathological abnormalities are elevated serum amylase and lipase.(1) Hyalinizing pancreatic adenocarcinoma is a form of EPC, and the main differential diagnoses are other variants of EPC, such as anaplastic (undifferentiated) EPC or pancreatic acinar or ductal carcinomas.(4) Pancreatic acinar cell carcinomas are further classified histologically as well-differentiated, which are less invasive, or poorly-differentiated, which tend to metastasize or invade adjacent tissue. One recent report found that loss of expression of claudin-4, a tight junction integral protein normally expressed in canine pancreatic acinar cell membranes, may lead to cellular detachment, disorientation and invasion in poorly-differentiated EPCs. The same study suggested immunohistochemical staining for claudin-4 as a marker to distinguish well-differentiated from poorly-differentiated acinar cell carcinomas.(3) Canine hyalinizing pancreatic adenocarcinomas behave less aggressively than the other, more common variants of canine EPC. Dennis, et al. speculate that this more benign behavior may be secondary either to the hyaline matrix material mechanically or biochemically impeding malignancy, or to the degree of tumor differentiation (or both).(1)
In the sections submitted for the conference, there is a diffuse loss of cellular detail and differential staining within the tumor, and because the contributor observed that some sections contained neoplastic emboli within lymphatics this led several conference participants to speculate that the entire neoplasm could be infarcted.
References:
2. Espinosa de los Monteros A, Fern+â-ídez A, Mill+â-ín MY, Rodriguez F, Herr+â-íez P, Martin de las Mulas J. Coordinate expression of cytokeratins 7 and 20 in feline and canine carcinomas. Vet Pathol. 1999;36:179-190.
3. Jakab CS, Rusvai M, Demeter Z, G+â-ílfi P, Szab³ Z, Kulka J. Expression of claudin-4 molecule in canine exocrine pancreatic acinar cell carcinomas. Histol Histopathol. 2011;26:1121-1126.
4. Pavone S, Manuali E. Eleni C, Ferrari A, Bonano E, Carioli A. Canine pancreatic clear acinar cell carcinoma showing unusual mucinous differentiation. J Comp Path. 2011;145:355-358.