Signalment:
4-year-old, castrated male, Border Collie,
Canis familiaris, canineThe dog presented to OSU Small Animal Services for evaluation of progressive neurologic disease of two weeks duration. Initially, the left pupil was dilated and the dog was diagnosed with and treated for anterior uveitis. One and a half weeks later, the dogs condition rapidly deteriorated with the onset of weakness, lethargy, anorexia, and disorientation.
Gross Description:
The dog was in good body condition. There were no significant gross lesions of the thoracic, abdominal viscera, or eyes. There was a 3 x 2.5 cm soft, grayish-tan, fixed mass ventral to the thalamus which surrounded the optic chiasm and extended from the ventral temporal lobe rostral to the chiasm to the level of cranial nerve V caudally. Following formalin fixation and sectioning, the mass extended 3-4 cm into the overlying brain parenchyma, involving approximately the ventral third of the brain. The majority of the mass was positioned to the left of midline, causing deviation of normal structures to the right.
Histopathologic Description:
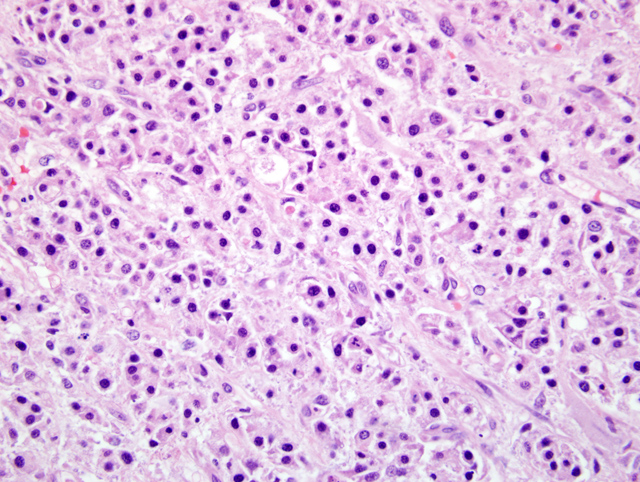
Diencephalon at optic chiasm. There is focally extensive infiltration of the ventral thalamus by a sharply demarcated but unencapsulated, multinodular, hypercellular mass. The mass is an admixture of cells exhibiting three distinct morphologies: 1) small round to polyhedral (germinal) cells with scant amphophilic cytoplasm which form dense packets separated by a thin fibrous stroma reminiscent of seminoma(
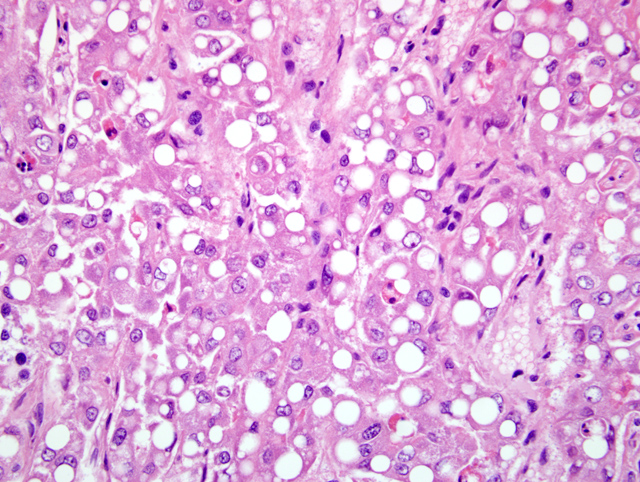
Fig. 4-3), 2) large polygonal (hepatoid) cells with abundant brightly eosinophilic cytoplasm which form broad sheets of anastomosing chords and which contain one or more large discrete clear cytoplasmic vacuoles that marginate the ovoid vesicular nuclei of the cells(
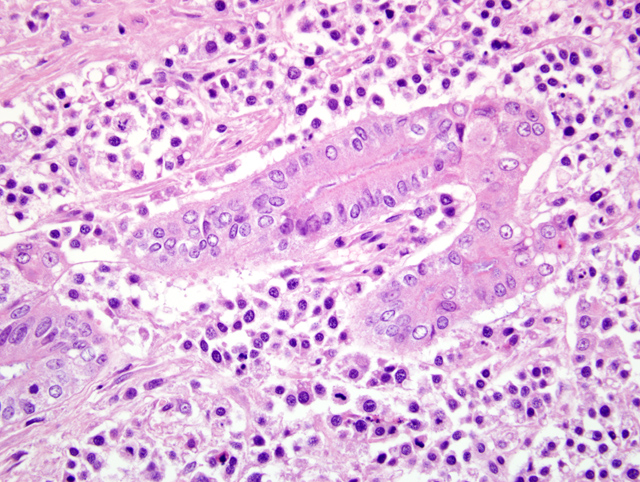
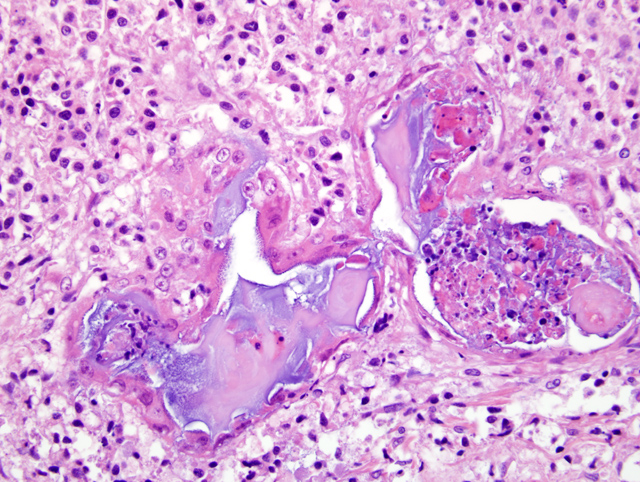
Fig. 4-4), and 3) large, closely-adherent polygonal (epithelial) cells with abundant eosinophilic cytoplasm and central round to ovoid vesicular nuclei which form irregular smaller sheets and chords(
Fig. 4-5), and exhibit occasional squamoid differentiation(
Fig. 4-6). Neoplastic cells of all three types exhibit a wide range of anisocytosis, anisokaryosis, and nucleoli of variable number and size. The epithelial cells occasionally keratinize and form small concentric whorls of keratin (keratin pearls). There are multifocal areas of coagulation necrosis- characterized by loss of differential staining, pyknosis, and karyorrhexis with accumulation of amorphous cellular and nuclear debris- and hemorrhage within the mass. Neoplastic cells, mainly of the hepatoid type, also appear to produce small lakes of homogeneous eosinophilic material (colloid) multifocally (not present in all sections). Mitotic figures are rare (<1 per 40 x field) though they are more common within the germinal neoplastic cell population than elsewhere. Occasional abnormal mitotic figures are noted. Brain tissue immediately adjacent to the mass is markedly compressed and has mild multifocal hemorrhage. There is no evidence of vascular invasion or of ventricular involvement (ventricle not present in all sections).
Regions of the neoplasm comprised of the epithelial and hepatoid cell populations were cytokeratin positive by immunohistochemistry.
Morphologic Diagnosis:
Diencephalon at optic chiasm: Suprasellar (Perichiasmatic) germ cell tumor with necrosis, hemorrhage, and local tissue invasion and compression
Lab Results:
- CBC/Profile: No abnormalities noted (performed by the referring veterinarian).
- Borrelia burgdorferi titer>/b>: Positive (performed by an emergency clinic, thought to be due to previous vaccination).
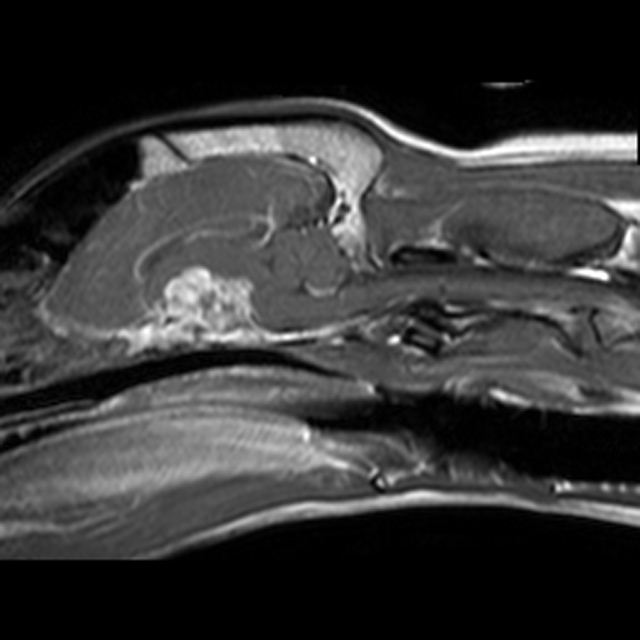
- Cranial MRI: Contrast-enhancing extra-axial mass ventral to the thalamus with dorsal displacement of adjacent structures. Meningioma suspected (performed by OSU) (Figs. 4-1, 4-2).
- Cerebrospinal fluid analysis: Mildly elevated protein levels and red blood cell count (performed by OSU).
Condition:
Suprasellar germ cell tumor
Contributor Comment:
The diagnosis of suprasellar germ cell tumor was made based upon the location and upon the presence of three diverse neoplastic cell populations within the tumor. Intracranial germ cell tumors can also occur within the pineal gland.(4,5) Human variants are further classified as seminoma, choriocarcinoma, entodermal sinus tumor, or teratoma based upon additional microscopic features of the tumor.(3) The cell of origin is presumed to be ectopic embryonic germ cells that have failed to migrate from the yolk sac to the developing gonad.(4,5) The neoplastic germ cells develop three distinct populations based upon morphology and growth pattern which are characteristic for intracranial germ cell tumors: 1) pleomorphic cells which form nests and sheets reminiscent of seminomas (Germinomatous cells) 2) large polygonal cells with abundant cytoplasm which contain lipid vacuoles and form nests (Hepatoid cells), and 3) epithelial cells reminiscent of intestinal or respiratory epithelium which can exhibit acinar, tubular, or squamoid differentiation and frequent keratinization.(1,2,3,5) Epithelial elements are thought to represent teratomatous change within the tumor.(4) Colloid-containing follicles were a minor component in this case and mineralization which is common in intracranial germ cell tumors was not present.(1,4) The epithelial elements of the tumor in this case were positive for cytokeratin by immunohistochemistry. The neoplastic cells within suprasellar germ cell tumors are also reported to exhibit positive α-fetoprotein staining by immunocytochemistry.(4, 5) Clinically, middle-aged dogs are most commonly affected by this rare tumor, with breed predisposition in Doberman Pinschers.(5) Neurologic signs are acute in nature and are most commonly those of cranial nerve involvement (CN III and IV most frequently exhibit deficits, though CNII XI may be involved) and/or thalamic compression (lethargy and stupor), both of which were present in this case.(5)
JPC Diagnosis:
Brain, diencephalon at the level of the optic chiasm: Suprasellar germ cell tumor
Conference Comment:
Extragonadal germ cell tumors are uncommon in both domestic animals and humans.(5) Due to their location and pattern, suprasellar germ cell tumors must be distinguished from pituitary adenomas and craniopharyngiomas.(3) Germ cell tumors generally arise in either the pineal gland or next to the sella turcica.(5) In man, most tumors occur in the pineal region, in contrast to the [predominately suprasellar location in dogs.(5) In humans, in addition to staining for alpha-fetoprotein, these tumors also often stain with human chorinonic gonadotropin, and placental alkaline phosphatase.(5)
Grossly, these tumors are usually very large, gray to white, extramedullary masses attached to the ventral aspect and often compressing the diencephalon.(5) Often admixed within the trivariant neoplastic cells are aggregates of lymphocytes that form small accumulations within the neoplasm.(5)
References:
1. Capen, CC: Endocrine glands.Â
In Pathology of Domestic Animals, Volume 3, eds. Jubb KVF, Kennedy PC, Palmer N, 4th ed., pp. 346-347, Academic Press, Inc., San Diego, CA, 1993
2. Koestner, A, Bilzer T, Fatzer A, Schulman FY, Summers BA, Van Winkle TJ: Histological classification of tumors of the nervous system of domestic animals. pp.32-34, Armed Forces Institute of Pathology, Washington, DC, 1999
3. Maxie, MG, Youssef S: Nervous system.Â
In Pathology of Domestic Animals, Volume 1, eds. Jubb KVF, Kennedy PC, Palmer N, 4th ed., pp. 454, Academic Press, Inc., San Diego, CA, 1993
4. Meuten, DJ: Tumors in domestic animals. 4th Ed, pp. 623-623, 728. Iowa State Press, Ames, Iowa, 2002
5. Summers, BA, Cummings JF, de Lahunta A: Veterinary Neuropathology. pp. 384-386. Mosby-Year Book, Inc., 1995