Signalment:
Gross Description:
Eyes: unilateral corneal opacification (ca. 3mm in diameter) and exophthalmos
Skin: 2 ulcerations on the head (ca. 2cm and 1mm in diameter)
Gallbladder: congestion
Spleen: severely enlarged, with round margins, scattered white pinpoints through the parenchyma
Intestine: low amount of whitish pasty content
Histopathologic Description:
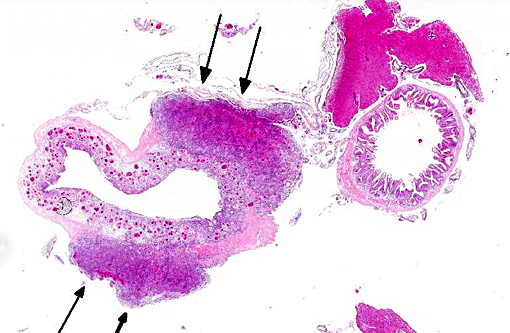
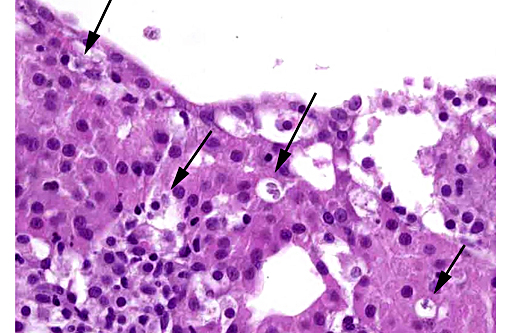
Stomach, focally extensively, the mucosa is replaced by moderate amounts of cell and nuclear debris (necrosis), large amounts of macrophages with abundant foamy cytoplasm, lymphocytes and plasma cells intermixed with multiple protozoan parasites. These parasites are pear-shaped, 4x10 μm, with one to two apical nuclei and two visible flagella on the other site (interpreted as Cryptobia iubilans). The same flagellates are also located in groups of up to 10 in the lamina propria, submucosa and serosa surrounded by aforementioned inflammatory cells and necrotic material. There is moderate proliferation of fibroblasts.
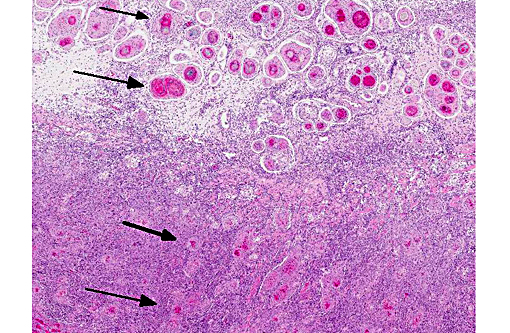
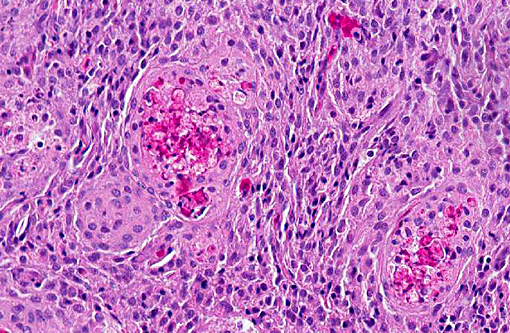
Multifocally to coalescing, the lamina propria, the submucosa and the serosa are severely thickened due to accumulation of large amounts of macrophages and lymphocytes, few plasma cells and eosinophil-like cells. Multifocally, mainly in the submucosa, granulomas are formed with central necrosis, marginating epithelioid macrophages, lymphocytes and fibroblasts.
In the adjacent perivisceral fat tissue and the spleen there are the same granulomas formed. In one section of liver, multifocally in the bile ducts, there are elongated structures with a basophilic membrane, granulated cytoplasm and multiple internal oval to pear shaped structures, 2x4 μm, with one to two nuclei (myxozoan plasmodia).
Morphologic Diagnosis:
Stomach, ulcerative and granulomatous gastritis, focally extensive, severe with intralesional flagellates.
Mesenteric fat tissue, granulomatous steatitis, multifocal, moderate
Liver, myxozoan plasmodia in bile ducts
Lab Results:
Parasitology: negative
Bacteriology: mixed flora with Aeromonas sobria in kidney, spleen, liver, skin
Condition:
Contributor Comment:
The ovoid or elongated body, 19x5 μm, has an anterior flagellum 1.5 to 2 times body length extending from the flagellar pocket, which is shielded by a mobile anterolateral protrusion of the anterior end, the rostrum, appearing as a small lobe and evidently supported by the microtubules of the preoral ridge.(1) It tends to be more elongated in early infection and more oval, tear-drop shaped or round in chronic infections.(2)
In transmission electron microscopy the flagellates are present in vacuoles (parasitophorous vacuole) in host cells. They are members of the order Kinetoplastida based on the detection of a kinetoplast, paraxial rod (lattice-like structure along the axoneme in the flagellum), and a cytoskeleton composed of microtubules lying beneath the body surface.(2)
Granulomatous gastritis caused by Cryptobia iubilans has previously been reported in 15 species of Old World and New World cichlids. As differential diagnoses for granuloma formation, mycobacteriosis, fungal, rickettsial, other parasitic (amoeba, nematodes) infection or foreign bodies could be considered. In this case, Ziehl-Neelsen special stain for acid-fast bacteria was negative. Flagellates commonly found in the intestine of many cichlid species are members of the order Diplomonadida, family Hexamitidae, including Spironucleus spp and Hexamita spp. They are typically found in the lumen of the intestinal tract and do not incite a granulomatous response.(2)
Morbidity and mortality rates in an infected population of fish appear to be linked to many environmental and biological variables such as water quality, the presence of other parasites or bacteria, diet, species, and age of fish. There are no effective clinically proven treatments against C. iubilans infection.
In salmonids, the haemoflagellate Cryptobia salmositica causes a microcytic and hypochromic anaemia and the severity of the disease is directly related to the parasitemia.(3)
In salmonids susceptible to Cryptobia salmositica, a generalized inflammatory response with severe lesions in connective tissues and in the reticuloendothelial system, as well as microlesions appearing in the liver, gills, and spleen at 12 weeks after infection, followed by endovasculitis with mononuclear cell and extravascular parasite infiltrations was described.(4)
JPC Diagnosis:
Conference Comment:
Cryptobia spp. infections in fish colonies have severe consequence for the aquarist, whose often only option to combat the disease is to depopulate, as there are no treatments yet clinically proven to be effective.(2) Relatively little is known about this recently reported parasite of African cichlids. While C. iubilans is considered to be pathogenic, some researchers consider it a facultative organism which capitalizes on stressful conditions such as poor water quality or other parasitism.(2) Granulomatous gastritis is the most commonly reported lesion, but granulomatous disease is often observed in multiple organ systems simultaneously. Within some sections in this case, granulomas are present in the spleen and liver, while pancreatic atrophy and testicular degeneration is also often apparent. The second parasite described by the contributor is a myxosporean, of which many have an evolved relationship with their host and thus do not result in disease. The myxozoan was not observed on most participants' slides.
References:
1. Lom J and Dykova I. Protozoan Parasites of Fishes. 1992. Elsevier Science Publishers B.V. Amsterdam, Netherlands. pages 52-51.
2. Yanong RPE, Curtis E, Russo R, Francis Floyd R, Klinger R, Berzins I, Kelley K, Poynton SL. Cryptobila iubilans infection in juvenile discus. J Am Vet Med Assoc 2004; 224(10): 1644-1650
3. Woo PTK. Cryptobia (Trypanoplasma) salmositica and Salmonid Cryptobiosis. J Fish Dis 2003; 26: 627646
4. Woo PTK. Immunological and Therapeutic Strategies against Salmonid Cryptobiosis. J Biomed Biotech 2010; doi:10.1155/2010/341783