Signalment:
Gross Description:
Histopathologic Description:
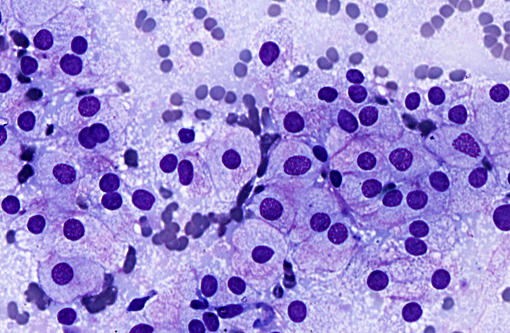
Cytologic description: Fine-needle aspiration of the mass was performed. The smear was highly cellular and consisted of monomorphic cells, most of which are in clusters. The cells had a round nucleus in pale abundant cytoplasm. The cytoplasm was mild to moderately vacuolated and small black pigment noted in a few cells. Cells showed mild to moderate anisocytosis and anisokaryosis, and mitotic figures were rarely seen.
From the left mandibular lymph node, similar morphologic cells were mainly acquired, and several small lymphocytes, plasma cells, and eosinophils were noted. On the smear of right mandibular lymph node, lymphoid cells, predominantly small mature lymphocytes with some lymphoblasts and plasma cells were seen. Scattered melanophages were also observed.
Morphologic Diagnosis:
1. Gingival mass: Malignant melanoma with metastasis to the left mandibular lymph node was suspected.
2. Right mandibular lymph node: Reactive lymph node.
Condition:
Contributor Comment:
JPC Diagnosis:
Conference Comment:
Differential diagnoses discussed include balloon cell melanoma, rhabdomyoma, granular cell tumor and oncocytoma. A definitive diagnosis is not possible without the use of immunohistochemistry, which was not performed by the contributor. Balloon cell melanoma is an uncommon variant of melanoma most commonly described in the skin in both domestic animals and humans, and in cats is often localized to the head. The cells are described as epithelioid, large and round, with abundant finely vacuolated cytoplasm that generally lacks pigment.(6,11) Glycogen (PAS positive) and lipid rich variants have been described, primarily in humans. Although the balloon cells may contain substances other than glycogen and other similar appearing non-melanocytic tumors may contain glycogen,(11) warranting a cautious interpretation of cytoplasmic features. The background of glycogen rich neoplasms is occasionally described as tigroid, referring to a vague tiger striping pattern imparted by background constituents.(4) Ultrastructural findings in balloon cell melanomas indicate the cytoplasmic vacuoles represent enlarged melanosomes. In addition to Melan A, balloon cell melanomas may stain for S-100 and neuron-specific enolase.(1,11)
Rhabdomyomas, oncocytomas and granular cell tumors have a similar cytologic appearance with eosinophilic granular material in the cytoplasm, comparable to what is seen in a subset of cells in this case. The similar cytoplasmic appearance in oncocytomas and rhabdomyomas is related to the presence of large numbers of mitochondria, and in granular cell tumors is postulated to be due to metabolic abnormalities and accumulation of lysosomes.(5) Rhabomyomas are benign tumors of striated muscle and may occur in the larynx and tongue of domestic animals. Cells may have abundant cytoplasmic glycogen, suggested by PAS positivity.(7) Oncocytomas are epithelial or neuroendocrine origin neoplasms which arise from oncocytes or oxyphil cells, and are described in the larynx of young dogs. The exact origin of granular cell tumors is unclear but they primarily occur in the oral cavity and have been conjectured to be of Schwann cell origin. Rhabdomyomas and oncocytomas have benign behavior, and the behavior of granular cell tumors is not well defined. Both rhadomyoma and oncocytoma have large pale cells with granular or foamy cytoplasm. The nucleus of oncocytoma is central, while the nucleus of rhadomyoma may be central or peripheral and both have finely clumped chromatin and a single indistinct nucleolus. Multinucleate cells may be seen in rhabdomyoma. The indistinct nucleolus is a feature which may help distinguish them from balloon cell melanoma. Granular cell tumors are variably sized but typically have abundant granular eosinophilic cytoplasm and an eccentric nucleus. Pleomorphism may be moderate in each of the three tumors. Additional diagnostics which may help differentiate the tumors include desmin positivity in rhabdomyoma, cytokeratin positivity in oncocytoma and PAS positivity (diastase resistance) in granular cell tumor.(2)
References:
1. Blanchard TW, Bryant NJ, Mense MG. Balloon cell melanoma in three dogs: a histopathological, immunohistochemical and ultrastructural study. J Comp Pathol. 2001; 125:254-261.
2. Burkhard MJ. Respiratory Tract. In: Raskin RE, Meyer DJ, eds. Canine and Feline Cytology. 3rd ed. St. Louis, MO: Elsevier; 2016:155-156.
3. Cangul IT, van Garderen E, van der Linde-Sipman JS, van den Ingh TS, Schalken JA. Canine balloon and signet-ring cell melanomas: a histological and immunohistochemical characterization. J Comp Pathol. 2001; 125:166-173.
4. DeMay RM. The Art and Science of Cytopathology. Vol 2. 2nd ed. Hong Kong: American Society for Clinical Pathology; 2012:592.
5. Dunbar MD, Ginn P, Winter M, Miller KB, Craft W. Laryngeal rhabdomyoma in a dog. Vet Clin Pathol. 2012; 41(4):590-593.
6. Goldschmidt MH, Dunstan RW, Stannard AA, Tscharner CV, et al. Histological classification of epithelial and melanocytic tumors of the skin of domestic animals. Vol III. 2nd series. Washington D.C.: Armed Forces Institute of Pathology. 1998:38-39.
7. Hendrick MJ, Mahaffey EA, Moore FM, Vos JH, Walder EJ. Histological classification of mesenchymal tumors of the skin and soft tissues of domestic animals. 2nd series. Washington D.C.: Armed Forces Institute of Pathology. 1998:21.
8. Kao GF, Helwig EB, Graham JH. Balloon cell malignant melanoma of the skin. A clinicopathologic study of 34 cases with histochemical, immunohistochemical, and ultrastructural observations. Cancer. 1992; 69:2942-2952.
9. Mowat A, Reid R, Mackie R. Balloon cell metastatic melanoma: an important differential in the diagnosis of clear cell tumors. Histopathology. 1994; 24:469-472.
10. van der Linde-Sipman JS, de Wit MM, van Garderen E, Molenbeek RF, et al. Cutaneous malignant melanomas in 57 cats: identification of (amelanotic) signet-ring and balloon cell types and verification of their origin by immunohistochemistry, electron microscopy, and in situ hybridization. Vet Pathol. 1997; 34:31-38.
11. Wilkerson MJ, Dolce K, DeBey BM, Heeb H, et al. Metastatic Balloon Cell Melanoma in a Dog. Vet Clin Pathol. 2003; 32(1):31-6.