Signalment:
Histopathologic Description:
Morphologic Diagnosis:
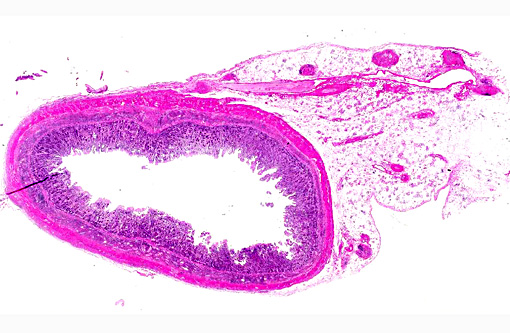
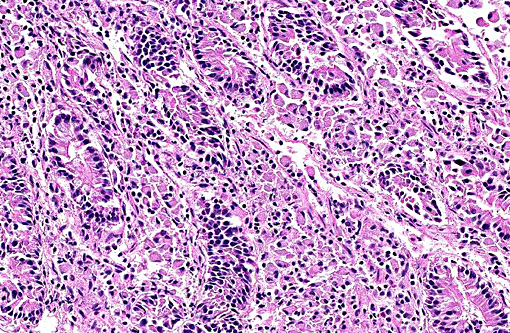
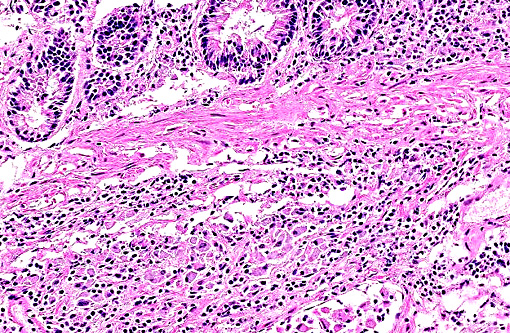
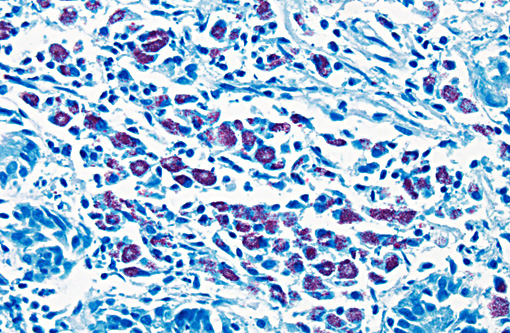
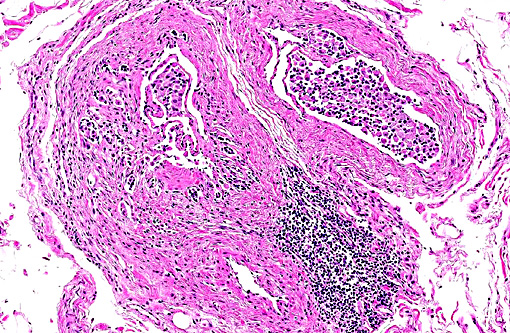
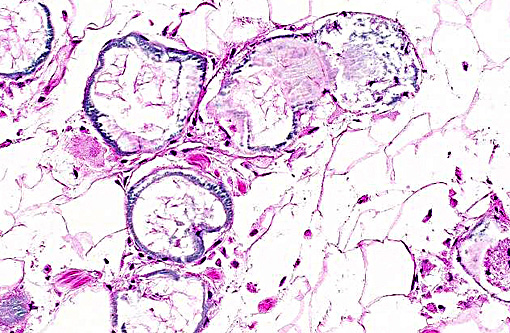
Small intestine: Enteritis, granulomatous, diffuse, severe, chronic with villous atrophy, lymphangectasia and macrophages containing acid fast bacilli seen with Ziehl-Nielson stain
Mesentery: Fat necrosis and mineralization, multifocal with lymphoplasmacytic perivasculitis
Condition:
Contributor Comment:
The route of disease transmission is fecal-oral route. After ingestion, the mycobacterium undergoes endocytosis by M cells of the dome epithelium over lymphoid follicles. It is proposed that integrin receptors on the apical surface of M cells bind fibronectin-opsonized bacteria, facilitating phagocytosis by these cells.(7) From M cells, the mycobacterium is transported in vacuoles to macrophages in subepithelial and intraepithelial areas of Peyers patches and lamina propria.(1,2) After uptake by macrophages, the bacteria resist the degradative and killing mechanisms of the macrophage via sulphatide production, which prevents phagosome-lysosome fusion, escape from the phagosome into the cytoplasm, glycolipid-mediated inhibition of nitric oxide production, and inhibition of the respiratory burst and oxidative killing mechanisms by superoxide dismutase and glycolipid production.(1)
Ovine Johnes disease has been noted as a problem in Australia and Europe. The disease in sheep can have three different forms with majority of the animals being asymptomatic. Among the clinically affected sheep, 30% are affected by paucibacillary (tuberculoid) form characterized by large number of T- lymphocytes, fewer eosinophils, macrophages and fewer bacteria in the gut. The rest of 70% have multibacillary (lepromatous) form with high levels of bacteria along with epithelioid macrophages and B lymphocytes infiltration,(5-8) as seen in this case. What determines the outcome of clinical disease is not entirely understood but various factors are implicated including the size of the infective dose, route of infection, mycobacterial strain virulence,(11) local and systemic immune status and age of the host, host resistance genes affecting antigen presentation and intracellular killing, and environmental factors.
In paratuberculosis, cell mediated immunity (CMI) plays a critical role in development of lesions and onset of clinical disease.(1,2) CMI develops relatively early in infection and, if effective, will lead to clearance of organisms and a resistant state.(1) The paucibacillary form is mediated by Th-1 response where bacterial growth within infected macrophage is controlled by IFN-γ and TNF-α production. The mulitibacillary form is mediated by Th-2 response with high production of IL-10 and little IFN-γ secretion and hence less control of intracellular bacterial growth.(5,8) It is interesting to note that the asymptomatic sheep are infected with mycobacterium but do not show any clinical or pathologic symptoms. The mechanism of disease resistance in asymptomatic animals is obscure. This differential activation of immune response to mycobacterium is speculated to be due to innate receptor engagement and signaling. Recently it is shown that different forms of sheep paratuberculosis have differential expression of pattern recognition receptors5 , including Toll-like receptors.(10)
JPC Diagnosis:
1. Intestine: Enteritis, granulomatous, diffuse, marked, with villar blunting, lymphangitis, and crypt loss.
2. Intestine: Fat necrosis with saponification.
Conference Comment:
The contributor discusses the pertinent differences of the cell-mediated immune response in relation to the two forms of disease, and we confirmed the lepromatous form in this case by repeating the acid-fast stains which revealed numerous intrahistiocytic bacteria. Clinical disease occurs due to the abundant granulomatous inflammation, and the lesions are often restricted to the ileum,(12) though the transmural granulomatous infiltration may also be observed in the colon and the organism has been cultured from a variety of organs.(1) Grossly the mesenteric lymph nodes are always enlarged and the classical intestinal change of diffuse mucosal thickening into transverse rugae is usually present in cattle.(1) In sheep and goats, the disease is characterized by chronic wasting and submandibular edema due to hypoproteinemia; the feces is usually normal in consistency and the gross enteric lesions are minimal, often missed at necropsy.(1)
References:
1. Brown CC, Baker DC and Barker IK: Alimentary system. In: Jubb, Kennedy and Palmers Pathology of Domestic Animals, ed. Maxie MG, 5th ed., vol. 3, pp. 222-225; 285-286 Elsevier Saunders, Philadelphia, PA, 2007
2. Clarke CJ. The pathology and pathogenesis of paratuberculosis in ruminants and other species. J Comp Path 116:217-261, 1997.
3. Gelberg HB. Alimentary system and the peritoneum, omentum, mesentery, and peritoneal cavity. In: Zachary JF, McGavin MD, eds. Pathologic Basis of Veterinary Disease. 5th ed. St. Louis, MO: Elsevier Mosby; 2012:385-387.
4. Laurin EL, Chaffer M, McClure SL, Keefe GP. The association of detection method, season, and lactation stage on identification of fecal shedding in mycobacterium avium ssp. Paratuberculosis infectious dairy cows. J Diary Sci. 2015;98(1):211-220.
5. Nalubamba K, Smeed J, Gossner A, Watkins C, Dalziel R and Hopkins J. Differential expression of pattern recognition receptors in the three pathological forms of sheep paratuberculosis. Microbes Infect. 10 (6):598-604, 2008
6. Perez V, Garcia-Marin JF and Badiola JJ. Description and classification of different types of lesions associated with natural paratuberculosis infection in sheep. J Comp Path 114:107-122, 1996.
7. Sigurethard³ttir OG, Valheim M and Press CM. Establishment of Mycobacterium avium subsp. paratuberculosis infection in the intestine of ruminants Adv Drug Deliv Rev.19; 56(6):819-34, 2004.
8. Smeed JA, Watkins CA, Rhind SM and Hopkins J: Differential cytokine gene expression profiles in the three pathological forms of sheep paratuberculosis. BMC Vet Res. 14; 3:18, 2007.
9. Smith SL, Wilson PR, Collett MG, et al. Liver biopsy histopathology for diagnosis of Johnes disease in sheep. Vet Pathol. 2014;51(5):915-918.
10. Taylor DL, Zhong L, Begg DJ, de Silva K and Whittington RJ. Toll-like receptor genes are differentially expressed at the sites of infection during the progression of Johne's disease in outbred sheep. Vet Immunol Immunopathol. 15;124(1-2):132-51, 2008.
11. Verna AE, Garcia-Pariente C, Mu+â-¦oz M, Moreno O, Garc+â-¡a-Marin JF, Romano MI, Paolicchi F, and P+â-¬rez V. Variation in the immuno-pathological responses of lambs after experimental infection with different strains of Mycobacterium avium subsp. paratuberculosis. Zoonoses Public Health. 54(6-7):243-52, 2007.