Joint Pathology Center
Veterinary Pathology Services
Wednesday Slide Conference
2017-2018
Conference 18
February 7th, 2018
CASE III: V165/17 (JPC 4102987)
Signalment: 1.5-year-old, male, castrated, domestic shorthair (Felis catus), feline.
History: Plaques, erosions and erythema have been present bilaterally for one year on the concave pinna around the entrance to the ear canal. There has been no response to various treatments.
Gross Pathology: The inner aspect of the pinna is thickened by plaques covered by thick dark brown-black exudate which occludes the entrance to the ear canal.
Laboratory Results (clinical pathology, microbiology, PCR, ELISA, etc.):
None provided.
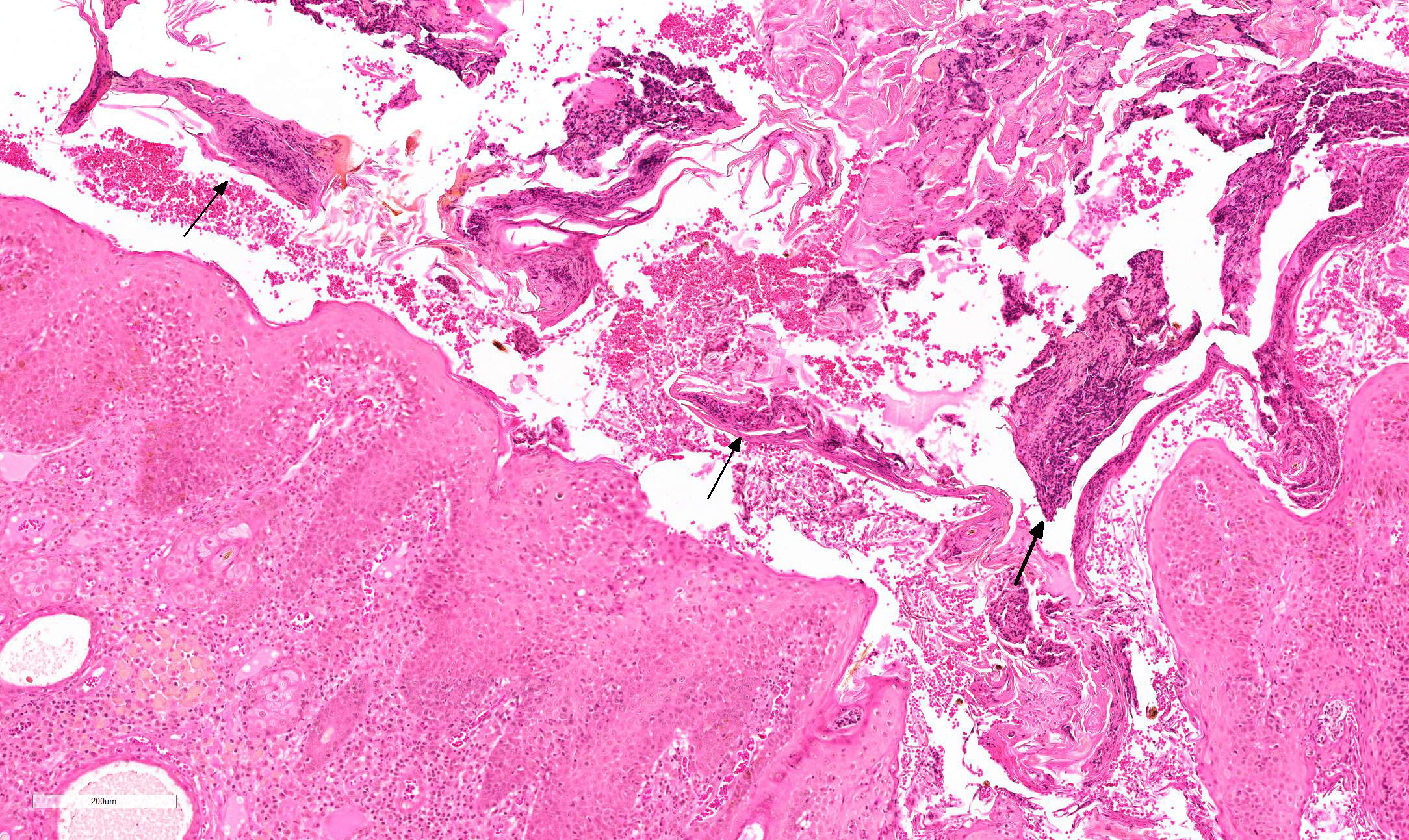
Microscopic Description:
The skin is covered by a thick crust composed of keratin and proteinaceous debris, large collections of lytic granulocytes (neutrophils and eosinophils), RBC and scattered bacterial colonies. There is severe diffuse hyperplasia of the epidermis and outer root sheath with widespread spongiosis. Dead keratinocytes with shrunken, angular, hypereosinophilic cytoplasm and pyknotic nuclei are present predominantly in the hyperplastic outer root sheath. They occur either as individual cells or form small groups and are often found in the upper layers of the epidermis or outer root sheath. There is prominent luminal folliculitis characterized by pronounced infundibular dilation, parakeratotic hyperkeratosis and formation of coalescing eosinophilic and neutrophilic pustules. The debris in the follicular lumen is continuous with the superficial crust. Keratinocytes with pale cytoplasm form an irregular layer below the disturbed stratum corneum of the most severely dilated hair follicle in this sample. A low number of eosinophils and probable lymphocytes migrate through the hyperplastic epidermis and outer root sheath. In the superficial and perifollicular dermis there is moderate to severe multifocal to coalescing infiltration of eosinophils, mast cells, neutrophils, a few lymphocytes, plasma cells and occasional macrophages with intracytoplasmic light brown granular pigment consistent with secretory material.
Contributor’s Morphologic Diagnosis:
Severe eosinophilic and mastocytic proliferative, hyperkeratotic and necrotizing dermatitis and folliculitis
Contributor’s Comment: This rare and distinctive skin disease of cats was first reported as “Proliferative necrotizing otitis of kittens” in the 2nd edition of Gross et. al..1 It was initially reported to affect cats <1 year-old, but a later publication describes cases also in adult cats.1,2
Clinically, the disease presents as bilateral, sharply demarcated, thick brown crusts usually on the inner surface of the proximal pinna and around the entrance to the ear canal.1,2,3 In some cases the vertical ear canal is involved.2,3 The proliferative tissue is friable leading to erosion, ulceration and in some case occlusion of the ear canal.1,2 The condition may regress spontaneously (by 1 to 2 years-old)1 or persist for a long time (e.g. 4.5 years)2. In the initial report, cats were described as indifferent to the lesions or demonstrated evidence of only mild pruritus when ulceration is present.1 More significant pruritus was noted in the cats of the 2nd report which had concurrent otitis due to bacterial or yeast infection.2
Gross et al. classify this condition as a necrotizing disease of the epidermis. Diseases in this group are characterized by death of keratinocytes either by necrosis or apoptosis. Since, the morphologic features of dead keratinocytes do not allow distinction between the two processes, the convention is that apoptosis is considered to be the underlying mechanism when death affects individual keratinocytes (e.g. erythema multiforme) and necrosis when death affects many confluent cells (e.g. toxic epidermal necrolysis). To complicate matters, dyskeratotic cells are also indistinguishable from dead keratinocytes.1 According to Mauldin et al. dead keratinocytes are limited to the outer root sheath and are not present in the interfollicular epidermis. The embedding of our samples is unfortunately oblique, but to the degree that we were able to pursue this point we tend to agree with Mauldin et. al. possibly with rare minor exceptions.
The cause of this condition is unknown. The possibility of viral infection was investigated by PCR and IHC but to date no evidence of viral involvement has been found.1,2 The two main references for this condition describe keratinocytes with abundant pale eosinophilic cytoplasm1,2, a finding which is present to a limited degree in the submitted sample (around the most dilated hair follicle). However, we did not identify enlarged nuclei with marginated chromatin without inclusion bodies.2
Individual keratinocyte death, presumably by apoptosis, suggests an immunologic basis1, and this is supported by the good response to treatment with Tacrolimus® (FK -506), an inhibitor of T-cell-mediated cytokines.2,5 Immunohistochemical analysis done on one case showed a close association between CD3+T cells and caspase-3-stained keratinocytes, which suggests that keratinocyte apoptosis is induced by epidermal infiltrating T cells, but the reason this occurs is unknown.5
JPC Diagnosis: Haired skin (external ear canal): Otitis externa, proliferative and hyperkeratotic with luminal folliculitis and keratinocyte apoptosis, domestic shorthair (Felis catus), feline.
Conference Comment: Proliferative and necrotizing otitis of kittens is a rare disorder that was first described in a 2007 academic journal by the moderator, Dr. Elizabeth Mauldin2, which characteristically presents as well-demarcated, erythematous plaques with adherent keratinaceous debris on the inner aspect of the pinna extending into the pre-auricular regions of the face. Although the gross appearance is unique and largely diagnostic, lesions can be easily confirmed via biopsy. Microscopically, the lesions are characterized by a markedly hyperplastic epidermis with brightly eosinophilic, shrunken keratinocytes (apoptotic or dyskeratotic) scattered subjacent to areas of prominent parakeratotic hyperkeratosis that contains layers of viable and degenerate neutrophils. Adjacent hair follicles may also be involved and are often plugged with keratinaceous debris and inflammatory cells.1,4
Histologically, this lesion is similar to hyperkeratotic erythema multiforme (EM), with several distinct differences: (1) affected keratinocytes are not routinely surrounded by lymphocytes (ie. satellitosis) and are only present in areas with prominent hyperkeratosis (suggesting that they may be dyskeratotic rather than apoptotic); and (2) there is minimal to mild epithelial hyperplasia and neutrophilic crusting, as evident with proliferative and necrotizing otitis. .1,4
Contributing Institution:
Department of Veterinary Resources,
Weizmann Institute of Science
Rehovot 76100, Israel
http://www.weizmann.ac.il/vet/
References:
- Gross TL et al. Skin Diseases of the Dog and Cat. 2nd ed. Oxford, UK: Blackwell Science; 2005:75, 79-80.
- Mauldin EA et al. Proliferative and necrotizing otitis externa in four cats. Vet Dermatol. 2007;18:370-377.
- Momota Y et al. Proliferative and necrotizing otitis externa in a kitten: successful treatment with intralesional and topical corticosteroid therapy. J Vet Med Sci. 2017;78(12):1883–1885.
- Stevens BJ, Linder KE. Pathology in practice. Proliferative and necrotizing otitis externa. J Am Vet Med Assoc. 2012;241(5):567-569.
- Vidémont E, Pin D. Proliferative and necrotising otitis in a kitten: first demonstration of T-cell-mediated apoptosis. J Small Anim Pract. 2010;51:599-603.