Signalment:
Gross Description:
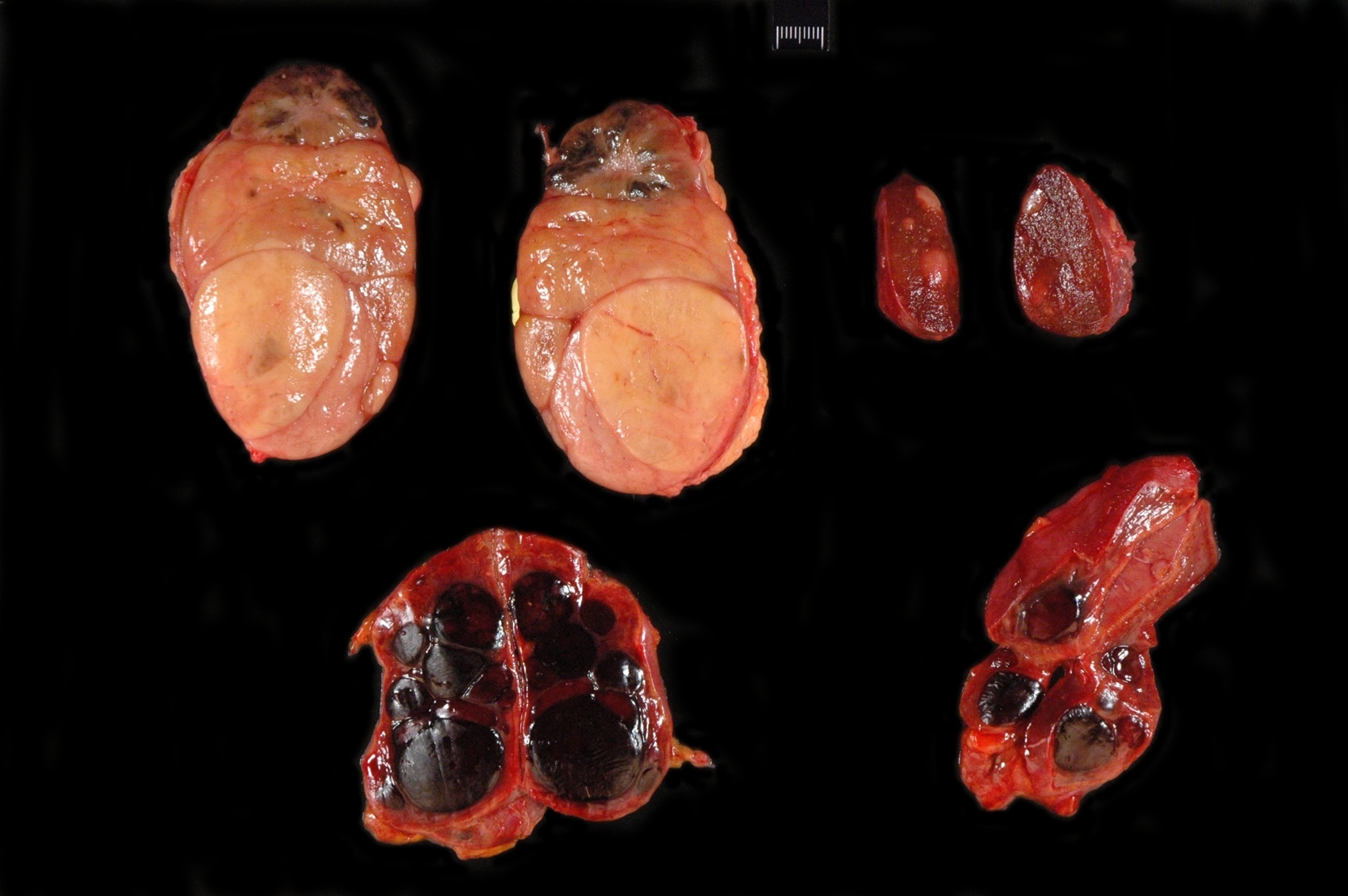
The right thyroid gland is markedly enlarged, measuring 12 x 7 x 5 cm. Its capsule is intact and the gland is freely moveable. On cut surface, almost all of the parenchyma is replaced by several tan, fleshy, expansile, multi-lobulated masses, the largest measuring 5 cm in diameter. One mass is very soft, friable and is mottled yellow and black. The left thyroid gland is moderately enlarged, freely movable, and measures 5 x 2 x 1.5 cm. On cut sections there are greater than twenty 0.2 - 1.0 cm soft, white, well-circumscribed spherical foci scattered throughout its parenchyma.
Bilaterally, affecting 80% of the left and 50% of the right adrenal gland, the medulla is replaced and expanded by red, fleshy, shiny, multifocal to coalescing, spherical masses that vary in size from 0.5-3.5 cm in diameter. The cortices, although slightly compressed, are intact.
Histopathologic Description:
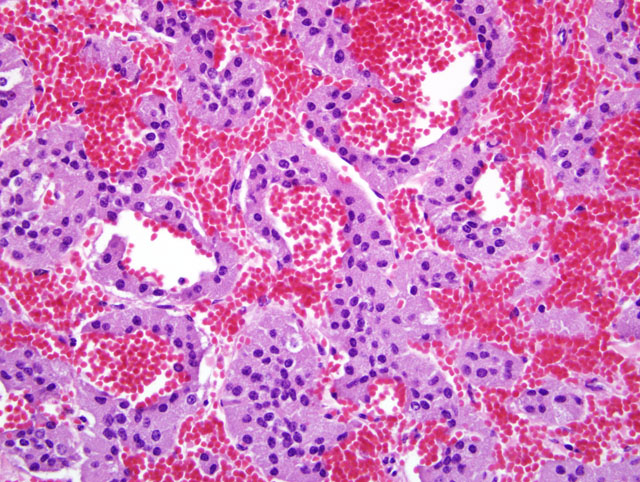
Adrenal glands, bilateral : Replacing much of the adrenal medulla and multifocally compressing the cortical parenchyma are multiple densely cellular, well circumscribed , and partially encapsulated masses composed of neoplastic polygonal cells arranged in nests and cords supported by a fine fibrovascular stroma. The neoplastic cells have oval nuclei, often with a single, dark, basophilic nucleolus, amphophillic, granular cytoplasm, and variably distinct cell borders. The mitotic rate averages 1 per high power field. Multifocally throughout the neoplastic masses, there are prominent blood filled sinuses.
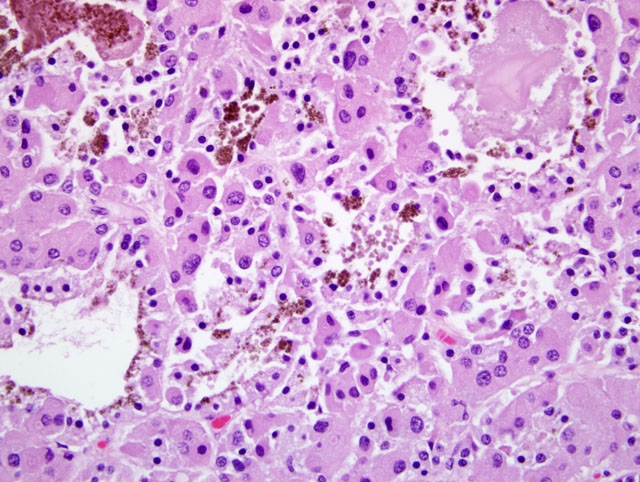
Right Thyroid Lobe (top tissue section): This section includes a portion of the 5 cm diameter mass described grossly and an adjacent, smaller multilobulated mass. The larger mass is a partially encapsulated, well circumscribed, expansile neoplasm composed of polygonal cells arranged in nests and cords. The neoplastic cells have moderate amounts of eosinophilic granular cytoplasm, round to oval nuclei that have vesicular to hyperchromatic chromatin, occasional eosinophilic intranuclear pseudoinclusions, and variably distinct cell borders. These cells demonstrate moderate to marked anisokaryosis and anisocytosis. The mitoses are less than 1 per high power field. Scattered randomly throughout the mass, accounting for approximately 40% of its composition, are entrapped and frequently compressed thyroid follicles, which are lined by low cuboidal cells with vacuolated cytoplasm and often pyknotic nuclei. A thin strip of thyroid parenchyma is compressed between the previously described mass and the smaller adjacent mass which is composed of disorganized aggregates of more uniform yet similarly shaped polygonal cells to those described in the larger mass. These cells demonstrate minimal anisocytosis and anisokaryosis. Entrapped follicles are also visible, accounting for 60-70% of this mass.
Left Thyroid Lobe (central tissue section): This section includes three of the masses seen grossly. These masses are partially encapsulated and compress the thyroid parenchyma. Otherwise these foci are similar to the smaller mass described in the right thyroid gland. Throughout the remainder of this tissue, there are aggregates of uniform yet similarly shaped polygonal cells to those already described that separate the thyroid follicles but lack any larger mass effect, encapsulation or compression affect of adjacent tissue. These aggregates of cells are interpreted to be hyperplastic foci.
Morphologic Diagnosis:
1. Adrenals, bilateral: Pheochromocytomas, multifocal to coalescing
2. Right thyroid lobe: C cell carcinoma and C cell adenomas
3. Left thyroid lobe: C cell adenomas and multifocal C cell hyperplasia
Condition:
Contributor Comment:
The masses in the thyroid are consistent with a transition from C cell hyperplasia to malignant neoplasia. The determination of carcinoma for the one mass is based on degree of cellular atypia rather than any overt evidence of invasion or metastasis. Initially, our top differential for these tumors was thyroid follicular cell carcinoma. However, immunohistochemical analysis of the tissue revealed that the neoplastic cells that form aggregates and sheets stain variably positive for calcitonin indicating that the tumor is of thyroid C (parafollicular) cell origin. The cells lining the follicles that are scattered multifocally within the masses are calcitonin negative. While the foci of hyperplastic cells are positive for calcitonin as are the medullary cells within the remnants of normal thyroid tissue. The latter are interpreted as normal C-cells.
Multiple endocrine neoplastic (MEN) syndrome is extensively described in humans and has multiple subtypes, many with defined genetic bases. This horse has both pheochromocytomas and C cell tumors and is therefore most consistent with MEN 2A wherein there is medullary thyroid carcinoma (C-cell neoplasia) and/or C-cell hyperplasia in nearly all cases as well as pheochromocytoma in approximately 50% of cases.(4) The cell of origin for medullary thyroid carcinoma in humans is derived from neural crest cells and is part of the amine precursor uptake and decarboxylation system (APUD). It is capable of calcitonin secretion, which is a marker for this tumor. Calcitonin levels were not measured in this horse. More common in bulls, C-cell tumors are also called ultimobranchial gland tumors due to their suggested origin from remnants of the ultimobranchial body, which is composed of cells that can differentiate into both C cells and follicular cells. The etiology of these tumors in bulls is unknown but there is a possible link with excessive long term dietary intake of calcium.(5) As in humans, bulls with C cell tumors often have pheochromocytomas and pituitary adenomas. This equine had multiple pheochromocytomas but no histologic evidence of a pituitary adenoma. De Cock et al. reported a case as well as retrospective data supporting the existence of MEN in horses. In their study, 4/72 horses had C-cell tumors only and 6/72 horses had both C-cell tumors and pheochromocytomas.(2) However, there is no mention that any of these C-cell tumors are carcinoma and their specific case is defined as a C-cell adenoma. Ueki et al. surveyed thyroid glands of aged horses and through use of immunohistochemistry found that the discrete white nodules found in 12/38 thyroid glands were consistent with thyroid C-cell adenomas. These nodules were only apparent when the thyroid was sectioned and involved only a small portion of the parenchyma. Histologically, the cells are described as mature with minimal atypia, unlike the neoplastic thyroid cells in our submission.(6)
JPC Diagnosis:
1. Adrenal gland: Pheochromocytoma; and multifocal medullary hyperplasia.
2. Thyroid gland, right lobe (per contributor): Parafollicular (C-cell) carcinoma; and parafollicular (C-cell) adenoma.
3. Thyroid gland, left lobe (per contributor): Parafollicular (C-cell) adenoma; and multifocal parafollicular (C-cell) hyperplasia.
Conference Comment:
- Nodular hyperplasia multiple small foci of well-demarcated, unencapsulated cells with similar histologic appearance to normal cells
- Adenoma solitary, well-demarcated, encapsulated, expansile mass which compresses adjacent tissue
- Carcinoma typically larger than adenomas, with evidence of capsular invasion, secondary foci of growth within the fibroadipose tissue surrounding the gland, intravascular tumor cells, metastasis, and cellular atypia
Thyroid parafollicular neoplasms are most common in aged bulls, rats and adult horses; these tumors are often functional in older bulls, though serum calcium may be within normal limits to mildly decreased owing to the relatively slow metabolic turn-over of bone and compensatory parathyroid gland hyperplasia.(1) It has been proposed that since calcitonin is released in response to hypercalcemia, the lesion in bulls could be due to prolonged ingestion of high calcium diets. Occasionally amyloid, which is believed to be derived from calcitonin, can be found within C-cell tumors in bulls. The typical immunohistochemical staining pattern for C-cell hyperplasia, adenoma and carcinoma is as follows:(3)
- C-cell hyperplasia consistently positive for calcitonin; variably positive for chromogranin A+B, synaptophysin, and neuron specific enolase (NSE); may be focally positive for somatostatin and bombesin
- C-cell adenoma consistently positive for calcitonin; variably positive for chromogranin A+B, synaptophysin, NSE and protein gene product 9.5 (PGP9.5); may be focally positive for somatostatin and bombesin
- C-cell carcinoma consistently positive for calcitonin; variably positive for chromogranin A+B, synaptophysin, and protein gene product 9.5 (PGP9.5); may be immunopositive for thyroid transcription factor 1 (TTF-1)
Among domestic animals pheochromocytomas occur most frequently in the ox and dog. Metastasis occurs in approximately half of all canine pheochromocytomas, with spread to the liver, regional lymph nodes, spleen and lungs. These malignant adrenal gland tumors are generally non-functional; when functional, clinical signs attributed to catecholamine excess include tachycardia, edema, cardiac hypertrophy, hyperthermia, arteriolar sclerosis and arteriolar medial hyperplasia.(1)
References:
2. De Cock HEV, MacLachlan NJ. Simultaneous occurrence of multiple neoplasms and hyperplasias in the adrenal and thyroid gland of the horse resembling multiple endocrine neoplasia syndrome: case report and retrospective identification of additional cases. Vet Pathol. 1999;36:633-636.
3. Kiupel M, Capen C, Miller M, Smedley R. Histological classification tumors of the endocrine system of domestic animals, 2nd series, vol. XII. Washington DC: Armed Forces Institute of Pathology; 2008:37-39, 46-47
4. Peczkowska M, Januszewwicz A. Multiple endocrine neoplasia type 2. Fam Cancer. 2005;4:25-36.
5. Seimiya YM, Takahashi M, Furukawa T, Mizutani K, Kimura K, Haritani M. An aged bull with concurrent thyroid C cell carcinoma, adrenal pheochromocytoma and pituitary chromophobe adenoma. J Vet Med Sci. 2009;71:225-228.
6. Ueki H, Koatari T, Oyamanda T, Oikawa M, Yoshikawa H. Non-functional C-cell adenoma in aged horses. J Comp Pathol. 2004;131:157-165.