Signalment:
Gross Description:
Diffusely the lungs were dark, red and heavy. The cut surface was similar and 100% of the lung was involved. The pericardial sac contained 10 mL of red fluid and diffusely there was minimal nodular thickening of the left atrioventricular valve.
Multifocally on the capsular and cut surface of the liver were numerous (approximately 10) raised, well-demarcated, yellow-white, soft, round nodules that were variably sized, ranging from 0.5 to 2 cm in diameter. Diffusely the pancreas was mottled dull grey-red and contained numerous raised, firm, round nodules that were up to 0.5 cm in diameter. Focally at the body of the pancreas, there was a larger, raised, poorly demarcated, yellow-white, firm, nodular mass that was 2 cm in diameter. The left kidney measured 42 x 30 x 20 mm and appeared normal. The right kidney and ureter were not present.
Morphologic Diagnosis:
Lab Results:
Condition:
Contributor Comment:
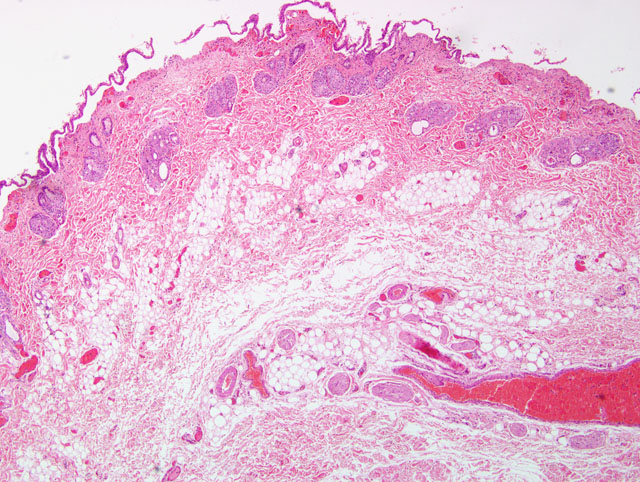
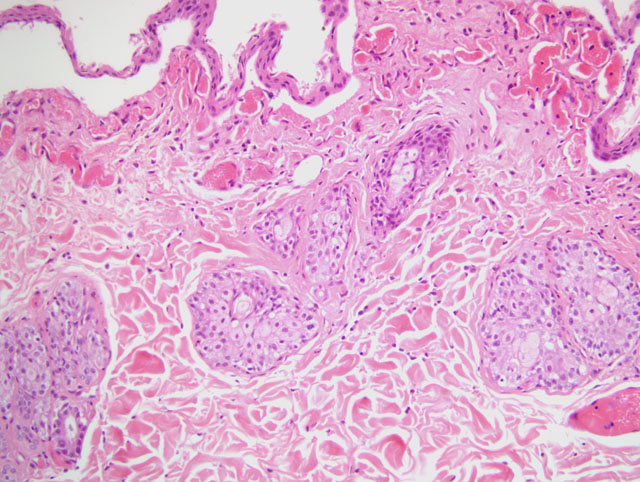
Histopathological examination of the skin consistently shows a non-scarring alopecia with characteristic marked follicular telogenization, miniaturization and atrophy, with similar adnexal atrophy. Other findings include mild epidermal acanthosis and hyperplasia with a hypo- or non-keratinized epidermis, and a mild, mixed, perivascular inflammatory infiltrate of the dermis, consisting of lymphocytes, macrophages and neutrophils.(3,4) In a recent report of feline skin biopsies complicated by Malassezia spp., histopathology from 7 of 15 cases was consistent with FPA. Although pancreatic carcinoma was confirmed in only four of these cats, it is possible that an indication of internal malignancy could be made when Malassezia spp. are detected in histopathology of cats with generalized skin disease.(2)
Neoplastic diseases of the exocrine pancreas and biliary tree are rare in the cat. The prognosis for these is generally poor since at the time of diagnosis the disease has often metastasized to distant sites, such as the liver, lymph nodes and lungs, as well as possibly local seeding to intraperitoneal sites. Twelve of the fourteen cats reported in the literature died or were euthanized within 8 weeks of onset of clinical signs.
JPC Diagnosis:
Conference Comment:
Differentiation between FPA and feline hyperglucocorticoidism (FHG) was discussed. Follicular atrophy is present in both conditions, but it is more striking in FPA and hair follicles in FHG have increased tricholemmal keratinization (bright eosinophilic core in an atrophic follicle) and follicular hyperkeratosis. Sebaceous glands may be atrophied in FHG, but are usually normal in FPA. The most striking feature of FHG is profound dermal atrophy, whereas the dermis is normal in FPA. FPA is also characterized by acanthosis with parakeratotic hyperkeratosis.(1)
In addition to FPA, other paraneoplastic skin lesions include feline thymoma-associated exfoliative dermatitis, nodular dermatofibrosis, feminization syndrome associated with Sertoli cell tumors, superficial necrolytic dermatitis and paraneoplastic pemphigus, all of which are described in an excellent review article.(5) Nodular dermatofibrosis occurs primarily in the German Shepherd Dog and is associated with renal cystadenomas or cystadenocarcinomas and uterine leiomyomas.(5) Superficial necrolytic dermatitis occurs more commonly due to hepatopathy or diabetes mellitus, but it has also been associated with a glucagonoma.(5) Paraneoplastic pemphigus is extremely rare.
References:
2. Mauldin EA, Morris DO, Goldschmidt MH: Retrospective study: the presence of Malassezia in feline skin biopsies, a clinicopathological study. Vet Dermatol 13:7-13, 2002
3. Pascal-Tenorio A, Olivry T, Gross TL, Atlee BA, Ihrke PJ: Paraneoplastic alopecia associated with internal malignancies in the cat. Vet Dermatol 8:47-52, 1997
4. Tasker S, Griffon DJ, Nuttall TJ, Hill PB: Resolution of paraneoplastic alopecia following surgical removal of a pancreatic carcinoma in a cat. Jour Small Anim Pract 40:16-19, 1999
5. Turek MM: Cutaneous paraneoplastic syndromes in dogs and cats: a review of the literature. Vet Dermatol 14:279-296, 2003