CASE 4: 933-17 (4116933-00)
Signalment:
14yo female spayed German Shepherd dog (Canis lupus familiaris)
History:
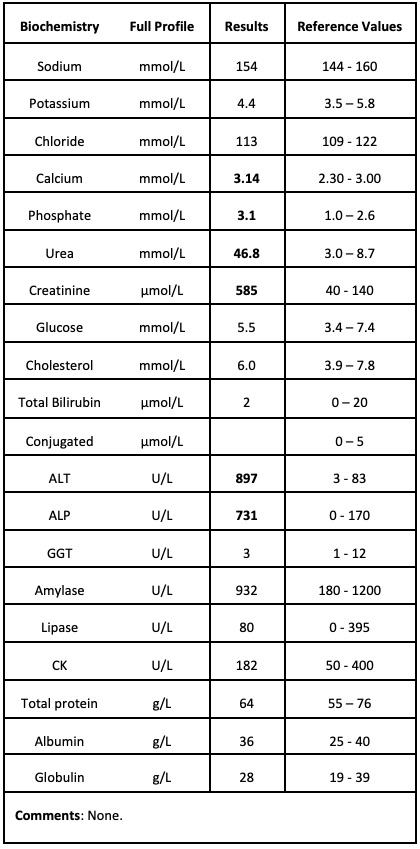
Presented anorexic for 5 days with polydipsia and intermittent vomiting over the previous week. The animal had lost 3.5kg in the past 3 months. The dog had previously been diagnosed with degenerative joint disease that was being treated with robenacoxib, amantadine, gabapentin, pentosane and fish oil supplementation. On clinical examination, the dog was tachycardiac and tachypneic with harsh lungs sounds. A marked azotemia was noted on a biochemistry profile with moderate elevation in ALT/ALKP (see laboratory results below). The dog was euthanized at the owner's request and submitted for post-mortem examination.
Gross Pathology:
The lungs were discolored red/purple with a slightly rubbery texture. Both kidneys were irregular in shape with expansion of the renal pelvis and bilaterally the renal papillae were overlayed by friable yellow material. Radiating yellow streaks were present in the renal medullae. Arising from the caudal left parietal and occipital bones of the skull, there was an irregularly shaped, moderately defined, multilobulated, hard mass approximately 6 cm x 4cm x 5cm which protruded from the exterior and interior surface of the skull. The underlying cerebellum was indented at the site of the mass.
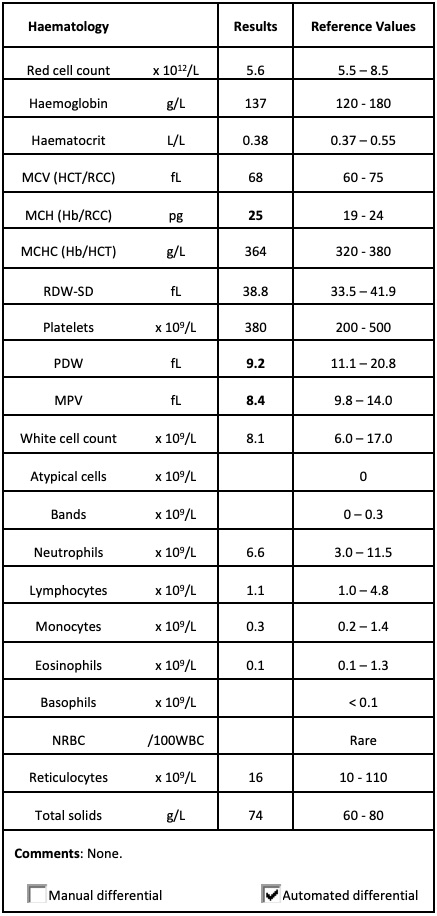
Laboratory results:
See inset tables.
Red cell morphology: Unremarkable.
White cell morphology: Unremarkable.
Platelet morphology: Unremarkable.
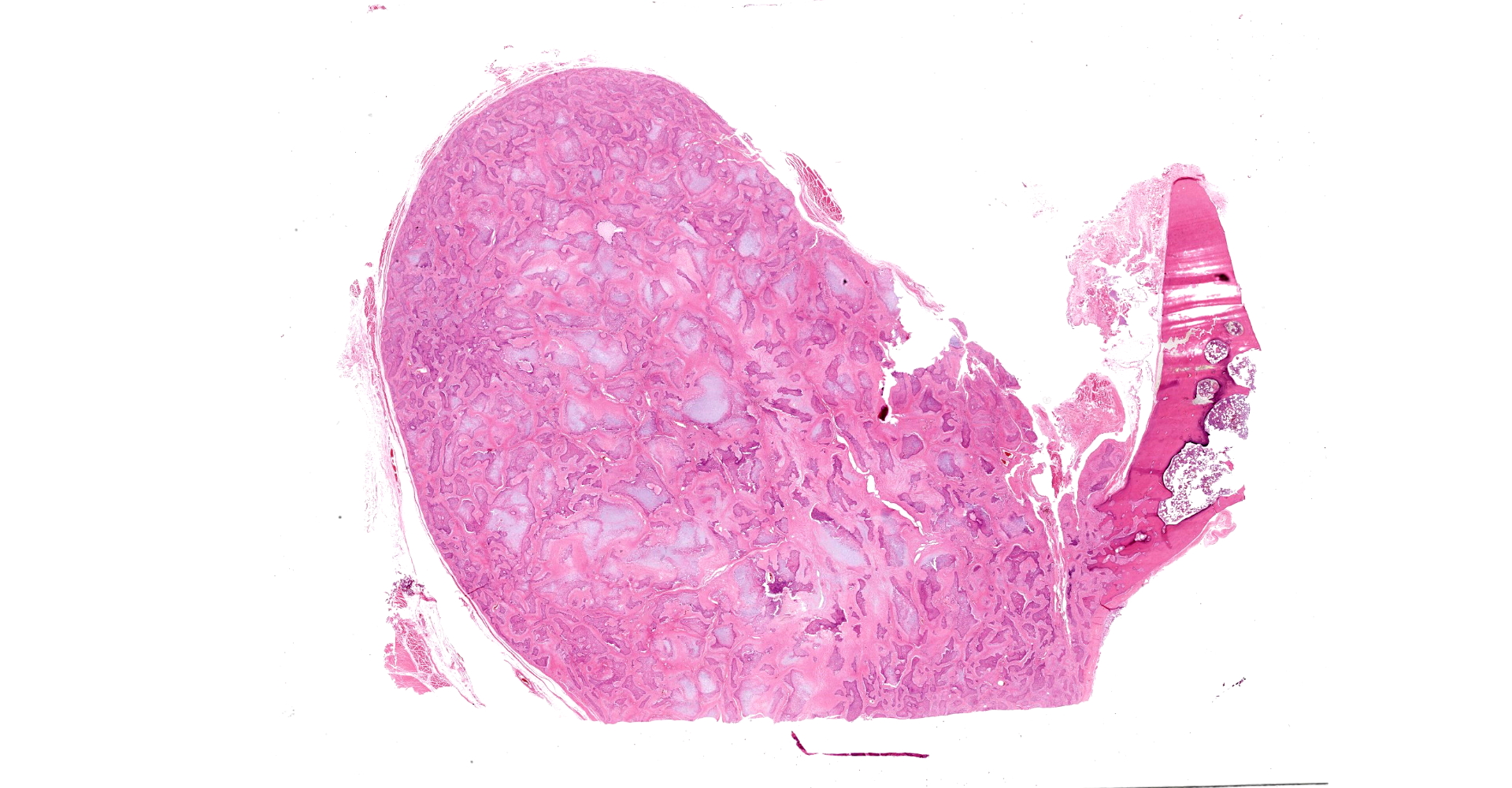
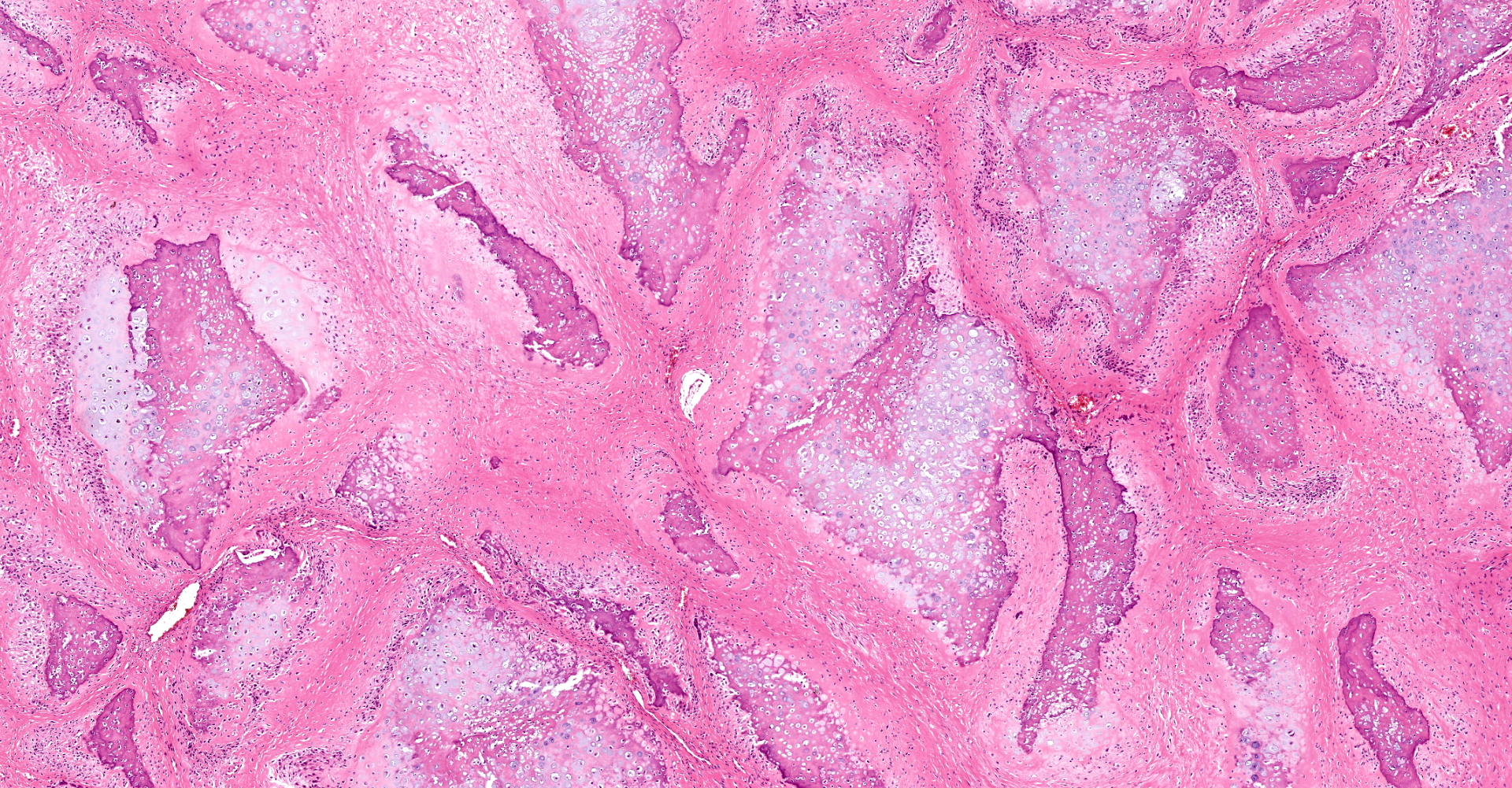
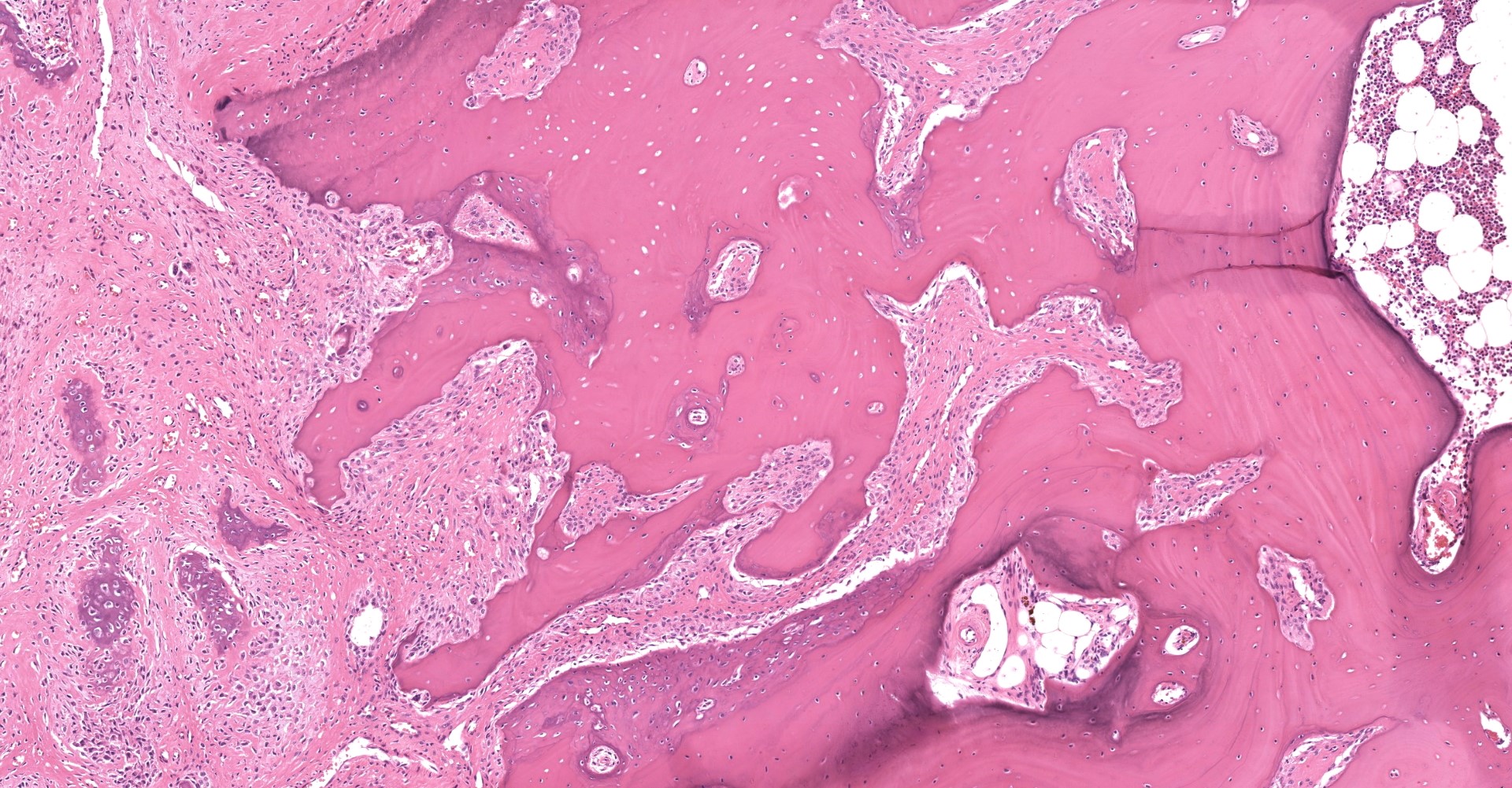
Microscopic description:
The mass is composed of irregular islands of hypercellular bone intermixed with a variable quantity of chondroid matrix containing cells within lacunae. Surrounding these islands there is a population of pleomorphic spindloid cells which have indistinct margins and lacy chromatin with a single central nucleolus. Occasionally there are giant cells within the population, but mitoses are rare. Dissecting between these regions there are septae of dense fibrous connective tissue. There is complete and active lysis of the adjacent calvarium, but the mass is well-circumscribed with no evidence of invasion.
Contributor's morphologic diagnosis:
Skull, parietal bone: Multilobular tumor of bone
Contributor's comment:
Multilobular tumor of bone (MTB, also known as multilobular osteochondrosarcoma, chondroma rodens, canine multilobular osteoma and chondroma, and calcifying aponeurotic fibroma) is an uncommon neoplasm that occurs most frequently in medium to large breed dogs, though it has also been reported in cats,1,7 a horse,6 and a ferret.3 Almost all MTB arise from the flat bones of the skull, but tumors arising from the chest have also been reported.5,7 MTB is typically slow-growing but locally invasive, and despite anecdotal reports of low metastatic potential, metastases were identified in 56% of cases in one study2, predominantly distributed within the lung, bone and soft tissues. Local recurrence is also common following excision.
MTB typically presents as a hard, well-defined and irregular nodule that arise from the external or internal surface of the skull, with a heterogenous gritty texture on incision that has been described as reminiscent of popcorn balls.2 The gross appearance is often suggestive of MTB, but differential diagnoses include osteoma, osteosarcoma, chondroma, chondrosarcoma, osteochondroma, osteochondromatosis, ossifying fibroma, meningioma, and craniomandibular osteopathy. The histological appearance of MTB is distinctive, characterized by a mosaic of well-differentiated mineralized and unmineralized cartilaginous and osseous tissue organized into discrete lobules separated by septa of fibrous connective tissue. A three-tier grading system has been developed for MTB8 based on the criteria of marginal invasion, lobular size, tissue organization, mitotic rate, cellular pleomorphism, and presence of necrosis. Grade III tumors were associated with faster metastasis and local recurrence following excision, as well as shorter survival time.
The tumor in this case was identified as an incidental finding, with the animal's clinical presentation relating to renal failure. Histological assessment of the kidneys identified severe chronic membranomesangial glomerulonephritis with interstitial fibrosis and acute renal papillary necrosis, potentially caused by NSAID therapy.
Contributing Institution:
JPC diagnosis:
Flat bone: Multilobular tumor of bone.
JPC comment:
As indicated by the contributor, multilobular tumor of bone is the preferred nomenclature, and these neoplasms may be either benign or malignant. The precise histogenesis of this neoplasm is yet to be determined, but research has provided a few clues. Most reported multilobular tumors of bone arise from either dermatocranium or viscerocranium, both of which are of intramembranous origin. Calvarial periosteal cambium cells grown in cell cultures have chondrogenic potential and may be the source of these tumors. There is also some evidence that the periosteal cambium layer of the calvarium has a different regulation mechanism than cambium cells in the axial and appendicular skeletal bones.9
Typical features of these neoplasms include irregular islands of hypercellular, disorganized bone with bland morphology. An outer fibrous septum surrounds an inner cambium-like cell layer, with a central core of cartilage and/or bone. They often have a gritty, nodular texture, and are well circumscribed. They are most often locally aggressive and invasive, with, as the contributor states, ~56% metastatic rate. When discovered, most metastatic disease is located in lung, bone, and soft tissue.
A recently described case of multilobular tumor of bone in a guinea pig was the first reported occurrence in a rodent. Similar to previously reported cases in other species, the affected guinea pig had an exophytic mass arising from the frontal bone, maxilla, and nasal bone. CT was performed to assist in determining surgical margins, which should be considered prior to antemortem surgical excision.4
References:
1. Bender S, Blazejewski S, Sánchez M: Diagnostic Imaging in Veterinary Dental Practice. Journal of the American Veterinary Medical Association 2014:244(6):651-654.
2. Dernell WS, Straw RC, Cooper MF, Powers BE, LaRue SM, Withrow SJ: Multilobular osteochondrosarcoma in 39 dogs: 1979-1993. J Am Anim Hosp Assoc 1998:34(1):11-18.
3. Hanley C, Gieger T, Frank P: What is your diagnosis? Multilobular osteoma (MLO). Journal of the American Veterinary Medical Association 2004:225(11):1665-1666.
4. Hatai H, Kido N, Ochiai K. Multilobular tumor of bone on the forehead of a guinea pig. J Vet Diag Invest. 2020;32(5):747-749.
5. Hay CW, Roberts R, Latimer K: Multilobular Tumor of Bone at an Unusual Location in the Axilla of a Dog. Journal of Small Animal Practice 1994:35(12):633-636.
6. Richardson DW, Acland HM: Multilobular osteoma (chondroma rodens) in a horse. J Am Vet Med Assoc 1983:182(3):289-291.
7. Rossetti E, Bertolini G, Zotti A: Multilobular tumour of bone of the thoracic wall in a cat. J Feline Med Surg 2007:9(3):254-257.
8. Straw RC, LeCouteur RA, Powers BE, Withrow SJ: Multilobular osteochondrosarcoma of the canine skull: 16 cases (1978-1988). J Am Vet Med Assoc 1989:195(12):1764-1769.
9. Thompson KG, Dittmer KE. Tumors of Bone. In: Meuten DJ, ed. Tumors in Domestic Animals, 5th Ed. Ames, IA:John Wiley & Sons, Inc. 2017:409.