Signalment:
15-year-old, castrated male, mixed breed, (
Canis familiaris) dogA 15-year-old castrated male mongrel dog
developed a mass in the left hemimandible around
the first molar tooth. The owner reported that the dog
pawed at its mouth. Two 1 cm x 2 cm incisional biopsy
specimens from the buccal and lingual aspects of the mass
were processed en toto for histologic examination by a
reference laboratory; the diagnosis was osteosarcoma.
One month later, the dog was admitted to the Purdue
University Veterinary Teaching Hospital for total left
hemimandibulectomy.
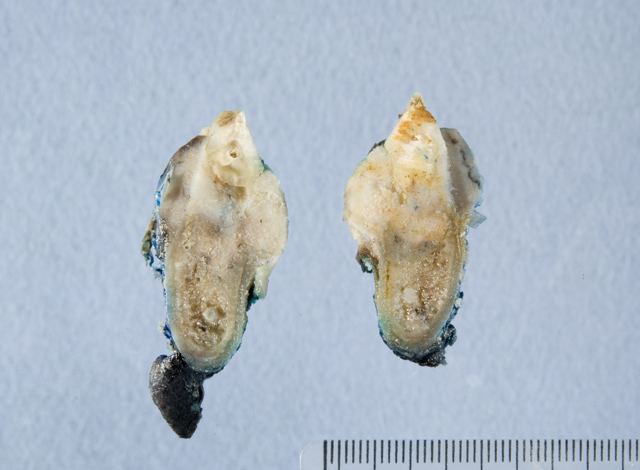
Gross Description:
A left hemimandibular surgical
specimen containing the entire mass had its margins painted
prior to immersion in 10% neutral buffered formalin and
submission to the Purdue University Animal Disease
Diagnostic Laboratory (ADDL), where the specimen was
transferred to a formic acid decalcifying solution. A firm
to hard fibrous and bony mandibular mass surrounded
the neck and roots of the first molar tooth and measured
about 2.5 cm from rostral to caudal margins and 2 cm from
medial to lateral aspects (
Figs. 2-1, 2-2). The mass on
cross-section consisted mostly of hard, white tissue that
infiltrated alveolar and cortical bone and adjacent soft
tissue (
Fig. 2-3).
Histopathologic Description:
The tumor consisted
of a spindle-cell proliferation resembling periodontal
stroma that appeared to be centered midway between
the neck of the tooth and its apex. At its apparent site
of origin, the tumor had provoked osteoclastic destruction
of alveolar bone, adjacent cortical compacta, periodontal
ligament and bone of the alveolar crest. Symmetric
growth of the mass expanded the lingual and buccal
borders of the hemimandible, again by stimulating
osteoclastic removal of the cortical compacta at a rate
that allowed development of a thin, incomplete shell of
periosteal new bone that partially contained the tumor.
At the gingival sulcus, the incomplete and partially
resorbed periosteal shell of reactive bone nearly abutted
the junctional gingival epithelium. Upward expansion of
the tumor into gingival lamina propria led to ulceration
and granulation tissue formation. On the buccal surface,
the tumor was also partially bound by a thin periosteal
shell of reactive bone that ended at the former level of
the alveolar crest, which had been replaced by neoplastic
tissue. Here, the tumor extended above the level of the
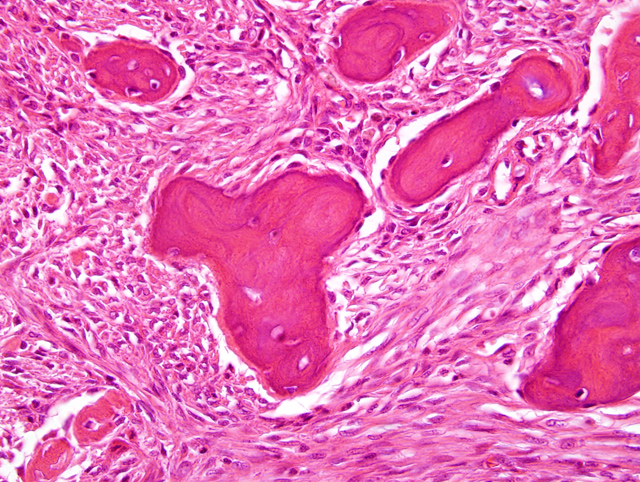
periosteal reaction into the gingiva. Neoplastic tissue was
composed of fusiform cells in scanty fibrous stroma with
light but diffuse infiltration by neutrophils. The fusiform
cells had an elongated oval nucleus, small nucleolus, no
mitotic figures in 15 high-power fields, and scanty pale
eosinophilic cytoplasm with indistinct cell borders (
Fig.
2-5). The stroma was moderately vascular with numerous
irregular trabeculae of osteoid and partially mineralized
woven bone. Bony trabeculae were bordered by one layer
of osteoblasts. A few osteoclasts were adjacent to bony
spicules. There was little fibrous collagen in tumoral
stroma; most of the Massons trichrome-stained collagen
was in the bony trabeculae. A preliminary diagnosis of
ossifying fibroma was reported with the final diagnosis to
follow examination of remaining (central) tissue.
Sections of the fully decalcified central portion of the
tumor were histologically similar to the initial peripheral
sections, except that 1 to 3 mitotic figures were found per
ten high-power fields. Neoplastic tissue was not found in
soft tissue ventral to the hemimandible or in mandibular or
soft tissue caudal to the mass. Histologic impression was
complete excision of an ossifying fibroma.
Morphologic Diagnosis:
Mandibular ossifying fibroma
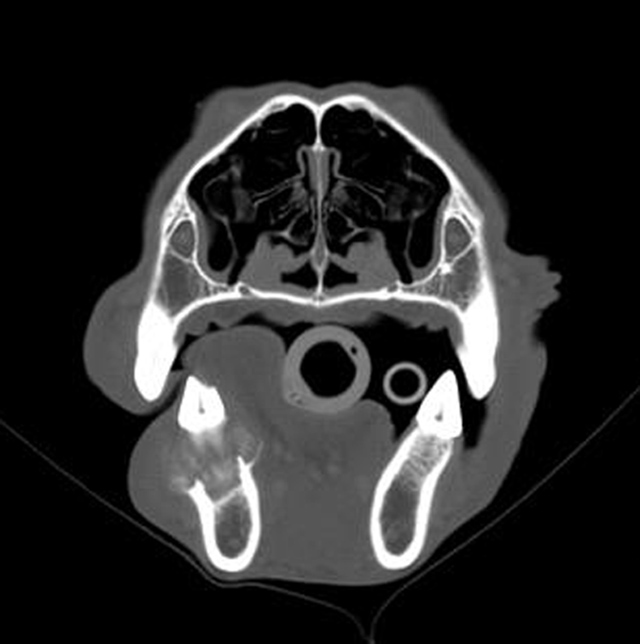
Lab Results:
No abnormalities were detected in
the available lateral radiographic view of the skull because
of superimposition of the hemimandibles. However, in
the computed tomographic (CT) scan, an expansile and
lytic lesion, about 1.8 cm in width and 2 cm from rostral to
caudal borders, was evident in the dorsal aspect of the left
hemimandible, surrounding the neck and roots of the first
molar tooth (
Fig. 2-4). The mass destroyed alveolar and
cortical bone, but had well-defined borders with a short
transition zone. There was slight swelling, but no postcontrast
enhancement of adjacent soft tissues. Thoracic
and abdominal radiographs were within normal limits and
free of evidence of metastatic neoplasia.
Condition:
Ossifying fibroma
Contributor Comment:
The case was reported as a
brief communication in Vet Pathol.
1 Benign fibro-osseous
proliferations of bone in veterinary species include
ossifying fibroma, osteoma, and fibrous dysplasia.
2,3
Osteomas are typically solitary osteosclerotic lesions
that arise from the surface of bones of the jaw or skull;
trabeculae of woven bone constitute the bulk of the tumor,
are rimmed by one layer of well-differentiated osteoblasts
and, in many cases, are oriented perpendicular to the
surface of the tumor.
3 Fibrous dysplasia
3 is a tumorlike
lesion that can involve one or multiple bones, often
in young animals. It arises within the bone, rather than
from the periosteal surface, and its ample fibrous stroma
contains only thin, curved trabeculae of woven bone. The
bony trabeculae are generally not rimmed by osteoblasts,
which distinguishes it from ossifying fibroma or osteoma,
and are regularly spaced but without orientation relative to
the periosteal surface.
Ossifying fibroma has histologic features that are
intermediate between those of osteoma and fibrous
dysplasia, although there can be overlap among the three
entities.
2 Ossifying fibroma is an expansile, lytic, and
invasive mass that develops within the bone, particularly
the mandible. Its bony trabeculae are rimmed by
osteoblasts as in osteoma, but are arranged haphazardly
and contribute relatively less to the fibro-osseous stroma.
Importantly, from a prognostic perspective, ossifying
fibroma must be differentiated from malignant tumors,
such as osteosarcoma. That distinction can be based on
the lower cellularity, bland cytologic features, and low
mitotic index of ossifying fibroma. Furthermore, bony
trabeculae of ossifying fibroma tend to be better developed
than in osteosarcoma and are bordered by a single layer of
osteoblasts that are distinct from the tumor cells. However,
histologic examination of excisional biopsy specimens
and knowledge of the anatomic location of the tumor may
be necessary for accurate diagnosis.
JPC Diagnosis:
Gingiva, tooth, and alveolar and
cortical bone: Ossifying fibroma
Conference Comment:
Ossifying fibromas are
most commonly reported in young horses, generally less
than one year of age, and usually present as a protruding
mass from the rostral mandible.
4 There have also been
reported cases in cats, dogs, and sheep.
4 In horses, the
differential diagnosis for ossifying fibroma includes
fibrous osteodystrophy, fibrous dysplasia, osteoma, and
osteosarcoma.
4 Fibrous osteodystrophy presents as a
symmetrical, bilateral lesion with numerous osteoclasts.
4
In fibrous dysplasia, bone spicules are not rimmed by
osteoblasts and are more uniform.
4 Osteomas are composed
of more normal appearing bone, while osteosarcomas have
invasive, pleomorphic cells with a higher mitotic index.
4
Osteomas are most common in horses and cattle and have
been reported as large as 14 cm in diameter.
3
Many tumors diagnosed as osteomas in dogs are actually
multilobular tumors of bone.
3 Histologically, the multilobular
tumor of bone consists of multiple vari-shaped
nodules of bone and/or cartilage at various stages of
differentiation separated by a fibrovascular stroma.
2,4
These tumors are slow growing but can be invasive and
may metastasize.
4 They have been reported in dogs,
cats, and horses.
4 Osteomas are dense masses of welldifferentiated
bone that protrude from bone surfaces.
References:
1. Miller MA, Towle HAM, Heng HG, Greenberg CB,
Pool RR: Mandibular ossifying fibroma in a dog. Vet
Pathol
45:203-206, 2008
2. Slayter MV, Boosinger TR, Pool RR, D+�-�mmrich K,
Misdorp W, Larsen S: Benign tumors.Â
In: Histological
Classification of Bone and Joint Tumors of Domestic
Animals, 2nd series, vol. 1, p. 5-7. Armed Forces Institute
of Pathology, Washington, DC, 1994
3. Thomson KG, Pool RR: Benign tumors of bone.Â
In:
Tumors in Domestic Animals, ed. Meuten DJ, 4th ed., pp.
248-255. Iowa State Press, Ames, IA, 2002
4. Thompson K: Bones and joints.Â
In: Jubb, Kennedy
and Palmers Pathology of Domestic Animals, vol 1 ed.
Maxie MG, 5th ed., pp.110-124. Elsevier, Philadelphia,
PA, 2007