WSC 2023-2024, Conference 21, Case 4
Signalment:
11-year-old, female spayed German shorthaired pointer (Canis familiaris)
History:
This patient initially presented for bilious vomiting and a pancreatic mass was subsequently identified on abdominal ultrasound and confirmed with computed tomography (CT). Partial pancreatectomy to excise a 15 mm diameter mass from the right distal limb of the pancreas was performed. The patient presented 6 weeks later for a recheck CT at which time an additional pancreatic mass was identified. Another partial pancreatectomy, this time of the left limb and body of the pancreas, was performed.
Gross Pathology:
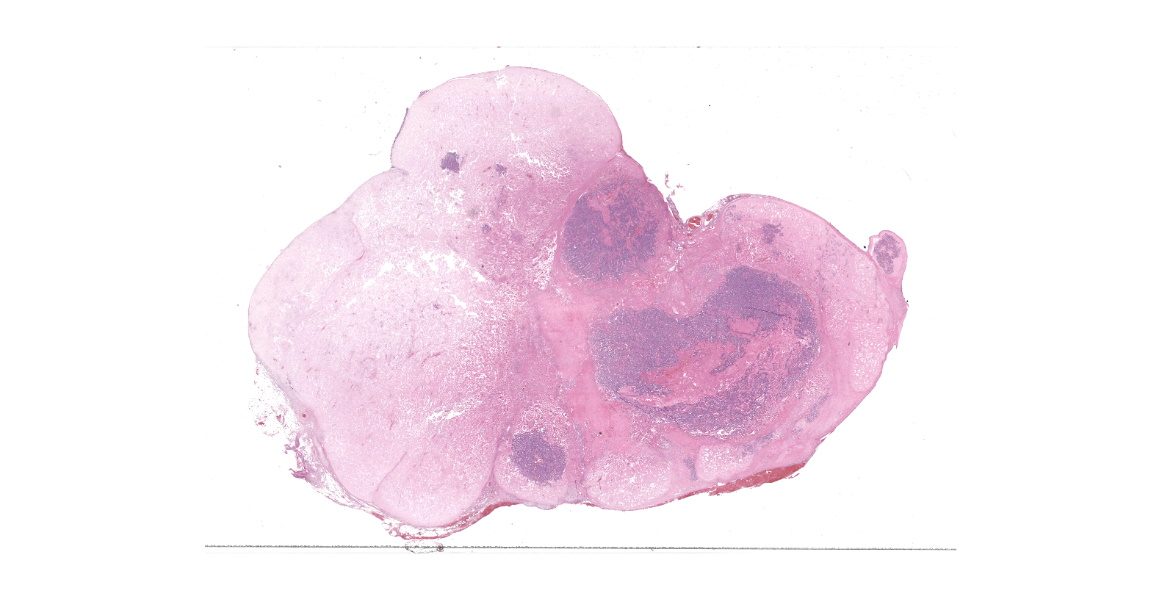
A formalin-fixed, 15 x 3 x 3 cm segment of the left limb and body of the pancreas was submitted for histologic evaluation. Near the proximal aspect was a rounded, 4 x 3 x 2.5 cm, light brown mass. The cut section revealed multifocal to coalescing rounded, smooth, firm, light brown, waxy nodular material (up to 1.4 x 1.2 x 1.2 cm diameter) with embedded and semi-firm brown tissue.
Microscopic Description:
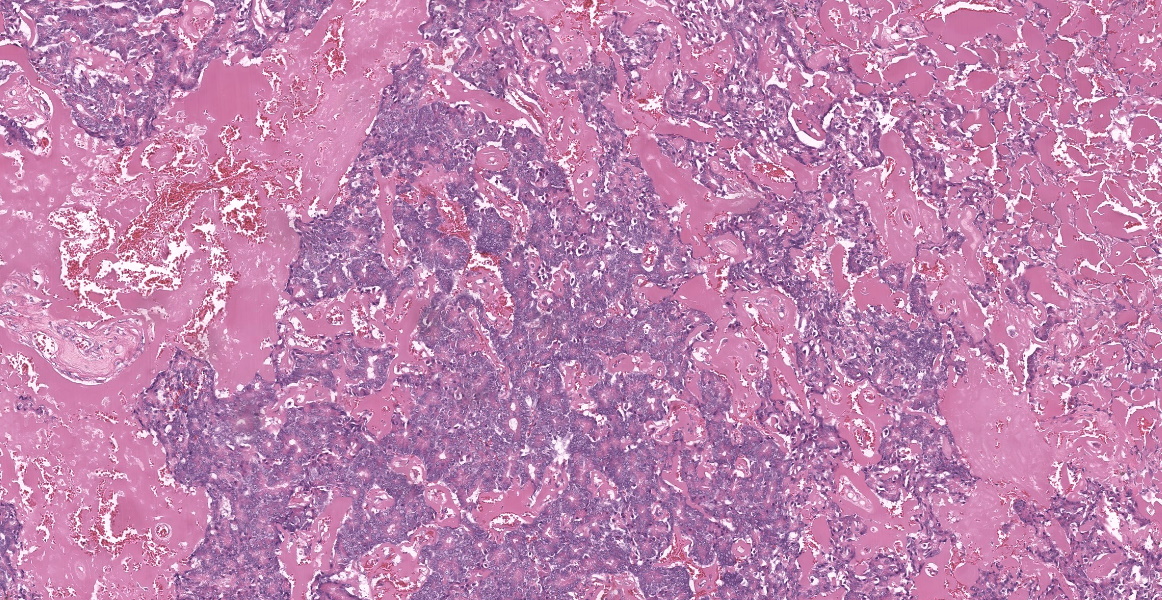
Pancreas: Markedly expanding, replacing, and effacing the pancreatic architecture and compressing resident pancreatic tissue, is a poorly-demarcated multilobular mass of neoplastic polygonal cells and extracellular matrix. Neoplastic cells form irregular acini and ducts and are embedded within and adjacent to an abundant, acellular, eosinophilic, hyalinized matrix that comprises approximately 30-70% of the mass (varied in different sections). Neoplastic epithelial cells have variably distinct cell borders, moderate to abundant brightly eosinophilic granular cytoplasm, and a large vesicular nucleus often with central single prominent nucleolus, but occasionally up to three nucleoli. Anisocytosis and anisokaryosis are moderate with frequent karyomegaly and 14 mitotic figures in 10 hpfs (2.37 mm2). Multifocally, ducts have lost cellular detail and contain eosinophilic cellular debris. Cellular debris and few macrophages with intracellular pyknotic debris are scattered throughout the neoplasm. Differentiation between overtly neoplastic cells and resident cells is limited in marginal areas where more normal tubules and acini are also in close proximity to the hyalinized matrix.
Contributor’s Morphologic Diagnosis:
Pancreas: Exocrine pancreatic adenocarcinoma, hyalinizing type.
Contributor’s Comment:
This pancreatic mass is consistent with a hyalinizing type of exocrine pancreatic carcinoma. A recent review of pancreatic carcinomas in the dog reports these tumors are rare with no clear sex-predilection and a potential breed predisposition in Airedale terriers.1 Clinical signs are typically non-specific and can include vomiting, inappetence, diarrhea, polyuria/polydipsia, and a palpable abdominal mass.1 The hyalinizing variant has only been reported in dogs, with most occurring in the right limb of the pancreas.3
The composition of the hyalinized matrix has not been fully characterized, though application of special and immunohistochemical stains to masses of this type have not been consistent with amyloid A, laminin, collagen, immunoglobulin, or alpha-1 antitrypsin.3
Types of recognized and reported variants of exocrine pancreatic carcinomas in the dog include acinar, ductal, hyalinizing, and mixed endocrine-exocrine.1,2 Growth patterns are described including acinar, solid, rosette, clear, mucinous, and tubulopapillary with variable differentiation.1,4 Acinar is most commonly reported in dogs, as compared to humans, in which exocrine pancreatic carcinomas are more often ductal, though differentiation can overlap within the same tumor.1 Exocrine pancreatic carcinomas have the potential for metastasis, especially to the liver and local lymph nodes.3 Evidence of metastasis was not identified in additional tissues submitted for this patient.
As cases are rare, no particular set of prognostic features has been established, though the hyalinizing variant may have better post-diagnosis survival times, especially if the patient survives the acute-post surgical interval.3 The patient in this case was alive at time of case submission, nearly seven months after initial diagnosis.
Contributing Institution:
Department of Population Health
and Pathobiology
North Carolina State University
College of Veterinary Medicine
Raleigh, NC 27607
https://php.cvm.ncsu.edu/
JPC Diagnosis:
Pancreas: Exocrine adenocarcinoma, hyalinizing type.
JPC Comment:
As the contributor notes, pancreatic neoplasia in dogs is rare, and the hyalinzing variant, so beautifully demonstrated by this case, is rarer still. Most canine pancreatic neoplasms are derived from the exocrine epithelium and are usually malignant, with clinical signs appreciated only after extensive local growth or metastasis to the liver, lymph nodes, or lymph nodes has occurred.3
Canine exocrine pancreatic carcinomas come in many varieties, with cuboidal, polygonal, or columnar cells of varying polarities and degrees of granulation forming tubules, acinar structures, or solid sheets of cells on stromal elements raning from delicate and fibrovascular to scirrhous. Histologic subcategories based on morphology are described for canine pancreatic neoplasias, though these subcategories currently have no confirmed prognostic significance or ability to predict biologic behavior.3
The hyalinizing variant of exocrine pancreatic carcinoma was first and most extensively described in a case series of six older mid-sized dogs; in most of these patients, the mass was present grossly as a single solitary mass, and most were discovered incidentally.3 As nicely demonstrated by this case, the feature that distinguishes the hyalinzing variant from a traditional exocrine pancreatic carcinoma is the presence of large contiguous areas of accumulated extracellular hyaline material that has the appearance, though not the staining or immunohistochemical properties, of amyloid.3 Neoplastic cells typically form tubules and are well-differentiated, with recognizable zymogen granules within the cytoplasm.3 In the initial case study, these histological features suggested a low-grade malignancy in all six cases, though some features of malignancy were noted, such as mild cellular atypia, frequent mitotic figures, and stromal invasion.3
As the contributor notes, based on the few reported cases of hyalinizing exocrine pancreatic adenocarcinoma, it is possible that this variant has a less aggressive course than its conventional counterpart. In contrast to conventional exocrine pancreatic adenocarcinomas, which have often metastasized or invaded at the time of diagnosis, in the initial descriptive case study of 6 dogs, metastatic disease was present in only 1 dog, and this dog lived for 16 months post-diagnosis.3 Speculating on the possible causes for this relatively indolent behavior, researchers posited that perhaps the unique accumulations of hyalinized matix within the tumor provided mechanical or biochemical impediments to the cell-matrix interactions required for tumor growth, invasion, and metastasis.3
Conference participants were struck by the abundant matrix that is the main histologic feature of this neoplasm. This matrix, together with the relatively differentiated neoplastic cells, made for an easy, though unfamiliar diagnosis. Discussion focused predominately on the nature of the matrix itself which, as noted, is of unknown composition. Participants evaluated a Masson trichrome, which stained the matrix an unusual gray-blue which was quite distinct from the vibrant blue staining of normal mature collagen. Evaluation of a Movat pentachrome stain revealed a deep yellow-orange color, most consistent with, but not specific for, collagen. While a tumor of first instance for most conference participants, the moderator noted that these tumors do occasionally appear in her diagnostic workload, including, an as-yet unpublished case in a cat.
References:
- Aupperle-Lellbach H, Törner K, Staudacher M, Müller E, Steiger K, Klop-fleisch R. Characterization of 22 canine pancreatic carcinomas and review of literature. J Comp Pathol. 2019;173:71-82.
- Belshaw Z, Bacon NJ, Foale RD, Mannion PM, Reuter R. Pancreatic mixed acinar-endocrine carcinoma in a dog. Vet Comp Oncol. 2005;3(3):145-148.
- Dennis MM, O'Brien TD, Wayne T, Kiupel M, Williams M, Powers BE. Hyalinizing pancreatic adenocarcinoma in six dogs. Vet Pathol. 2008;45(4):475-483.
- Pavone S, Manuali E, Eleni C, Ferrari A, Bonanno E, Ciorba A. Canine pancreatic clear acinar cell carcinoma showing an unusual mucinous differentiation. J Comp Pathol. 2011;145(4):355-358.