Signalment:
Histopathologic Description:
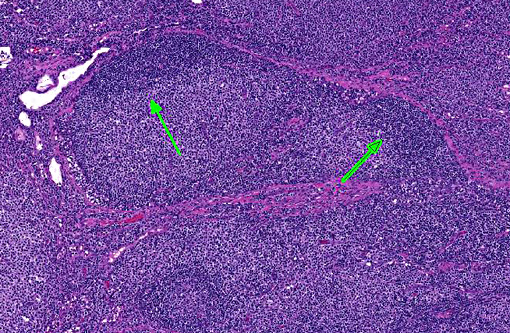
Immunohistochemical stains CD3, CD20 and CD79a were performed. The neoplastic cells have strong positive CD3 immunoreactivity. The peripheralized fading follicles have positive CD20 and CD79a immunoreactivity. This staining pattern confirms the diagnosis of a T-zone lymphoma.
Morphologic Diagnosis:
Condition:
Contributor Comment:
T-zone lymphoma first appeared in the Kiel classification with a description of a nodal lymphoma that occurs rarely in humans.(7,8) In 2008, a description was added to the human WHO (World Health Organization) classification as a morphologic variant of peripheral T-cell lymphoma not otherwise specified (PTCL-NOS), and is characterized by a clonal expansion of T-zone lymphocytes that exhibit a unique architectural and cytomorphologic pattern.(2,5) Human TZL comprise only 1.5% of all cases of PTCL-NOS.(5) Although the true incidence of canine TZL is unknown, two recent publications indicate that they are relatively common, comprising between 15.5 and 62% of all canine indolent lymphomas, which themselves are reported to have an incidence rate of 29% of all canine lymphomas.(2,5,8) Almost all cases of TZL occur in peripheral lymph nodes with a predilection for the mandibular node, and usually have a history of a single enlarged lymph node for as long as a year.(7) A higher incidence rate is observed in the golden retriever and shih tzu breeds, and in the majority of cases, a lymphocytosis is frequently reported at the time of diagnosis.(2, 5)
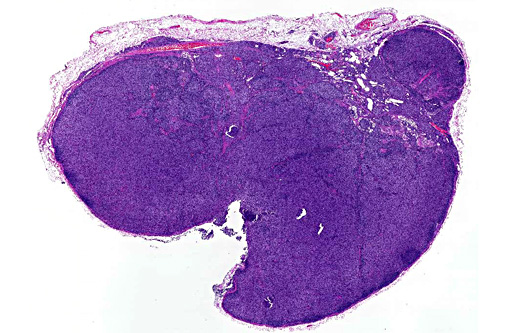
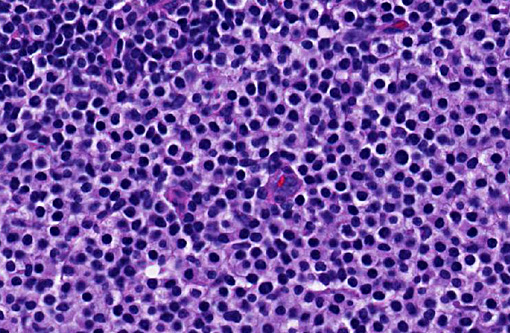
The WHO system of classification of canine lymphomas defines TZL as a nodal T-cell lymphoma, in which neoplastic cells expand the paracortex and medullary cords without effacement of the nodal architecture.(7) The architecture of TZL has a signature pattern that results from the expanding population of neoplastic T-cells which peripheralizes fading atrophied germinal centers in the outer cortex and medulla. The capsule is usually focally thinned, the peripheral sinuses are compressed, and postcapillary venules are prominent. The intervening areas of paracortex are expanded by a uniform population of small or intermediate sized lymphocytes. There is no extension of the neoplasm into the peripheral sinuses or perinodal tissue. Areas of empty sinus ectasia are observed in the later stages. Two subtypes are categorized based on the nuclear size of the neoplastic T-cells compared to the diameter of a red blood cell (RBC). TZL of small cells have nuclei that are 1-1.25 x RBC, and TZL of intermediate-sized cells are 1.5 x RBC. Neoplastic cells have distinct cell borders with abundant cytoplasm. The nuclei have frequent sharp shallow indentations, are hyperchromatic with little internal detail, and inconspicuous nucleoli. The mitotic index is low, usually 0-1 on most 40x fields.
TZL must be differentiated from small lymphocytic lymphoma of T or B-cell type and benign small lymphocytes that are diagnosed via fine-needle aspirates.(7) B-cell proliferations symmetrically surround germinal centers. Small lymphocytic lymphomas are not associated with fading germinal centers or sinus ectasia, and the nuclei do not have consistent nuclear indentations.
Immunohistochemistry and flow cytometry are powerful tools when differentiating TZL from benign nodules of hyperplasia and other nodal lymphomas. TZL cells have a solid CD3 positive immunoreactivity and are negative for CD79a and CD20.(5,7) A recent study demonstrated CD45 immunophenotyping using flow cytometry on peripheral blood and lymph node aspirates.(5) CD45 is a tyrosine phosphatase that has a complex role in the regulation of signaling through the T-cell receptor, and in the regulation of cytokine receptor activation. Neoplastic T-cells do not express CD45. To date, there is no normal CD45 negative T-cell counterpart described in mice or people, and no evidence of CD45 negative T-cells in the blood or lymph nodes in normal or reactive canine lymph nodes. The loss of CD45 expression appears to be correlated with malignant transformation of T-cells; however, the mechanisms involved are not known.
JPC Diagnosis:
Conference Comment:
Lymphoma can be readily diagnosed on fine needle aspirate; however, it is not yet possible to subclassify it by cytology alone. Aspirates of T-cell lymphomas do sometimes have a hand mirror morphology when smeared onto a slide which may allow the examiner to favor this classification.3,6 These cells are mentioned in other sources as reactive lymphocytes with plasmacytoid features, thus their presence should be interpreted with caution.(4)
References:
1. Avery A. Molecular diagnostics of hematologic malignancies. Top Companion Anim Med. 2009;24(3):144-150.
2. Flood-Knapik KE, Durham AC, Gregor TP, S+�-�nchez MD, Durney ME, Sorenmo KU. Clinical, histopathological and immunohistochemical characterization of canine indolent lymphoma. Vet Comp Oncol. 2013;11:272286.
3. Han JY, Kim JS, Kim DH, et al. Cytologic features of ascetic fluid complicated by small cell variant T-cell prolymphocytic leukemia-a case report. Korean J Cytopathol. 2008;19(2):168-172.
4. Rizzi TE, Cowell RL, Tyler RD, Meinkoth JH. Effusions: abdominal, thoracic and pericardial. Diagnostic Cytology and Hematology of the Dog and Cat. 3rd ed. St. Louis, MO: Mosby Elsevier; 2008:240-241.
5. Seelig DM, Avery P, Webb T, et al. Canine t-zone lymphoma: Unique immunophenotypic features, outcome, and population characteristics. J Vet Intern Med. 2014;28:878886.
6. Valli VE, Kass PH, San Myint M, Scott F. Canine lymphomas: Association of classification type, disease stage, tumor subtype, mitotic rate, and treatment with survival. Vet Pathol. 2013;50(5):738-748.
7. Valli VE, San Myint M, Barthel A, et al. Classification of canine malignant lymphomas according to the World Health Organization criteria. Vet Pathol. 2011;48:198211.
8. Valli VE, Vernau W, Lorimier LP, Graham PS, Moore PF. Canine indolent nodular lymphoma. Vet Pathol. 2006;43:241256.