Signalment:
16-year-old pony breed mare (
Equus caballus).The pony became ataxic one week before presenting at the clinic. The referring veterinarian found
neurological signs affecting the tail and hindlimbs. At the Norwegian School of Veterinary Science clinic,
neurological examination indicated that facial nerves (V and VII) were affected. Muscle tone in the tail and anus
was reduced. Hindquarter skin had areas of hypersensitivty and areas of reduced sensitivity. Severe ataxia was
found.
Gross Description:
In the gluteal region there was edema and hemorrhages centered on nerves. The lumbosacral
spinal cord (L5-S1) was firm and slightly irregular in thickness. There was hemorrhage in the epidural and subdural
spaces and dark hemorrhagic foci in the spinal cord.
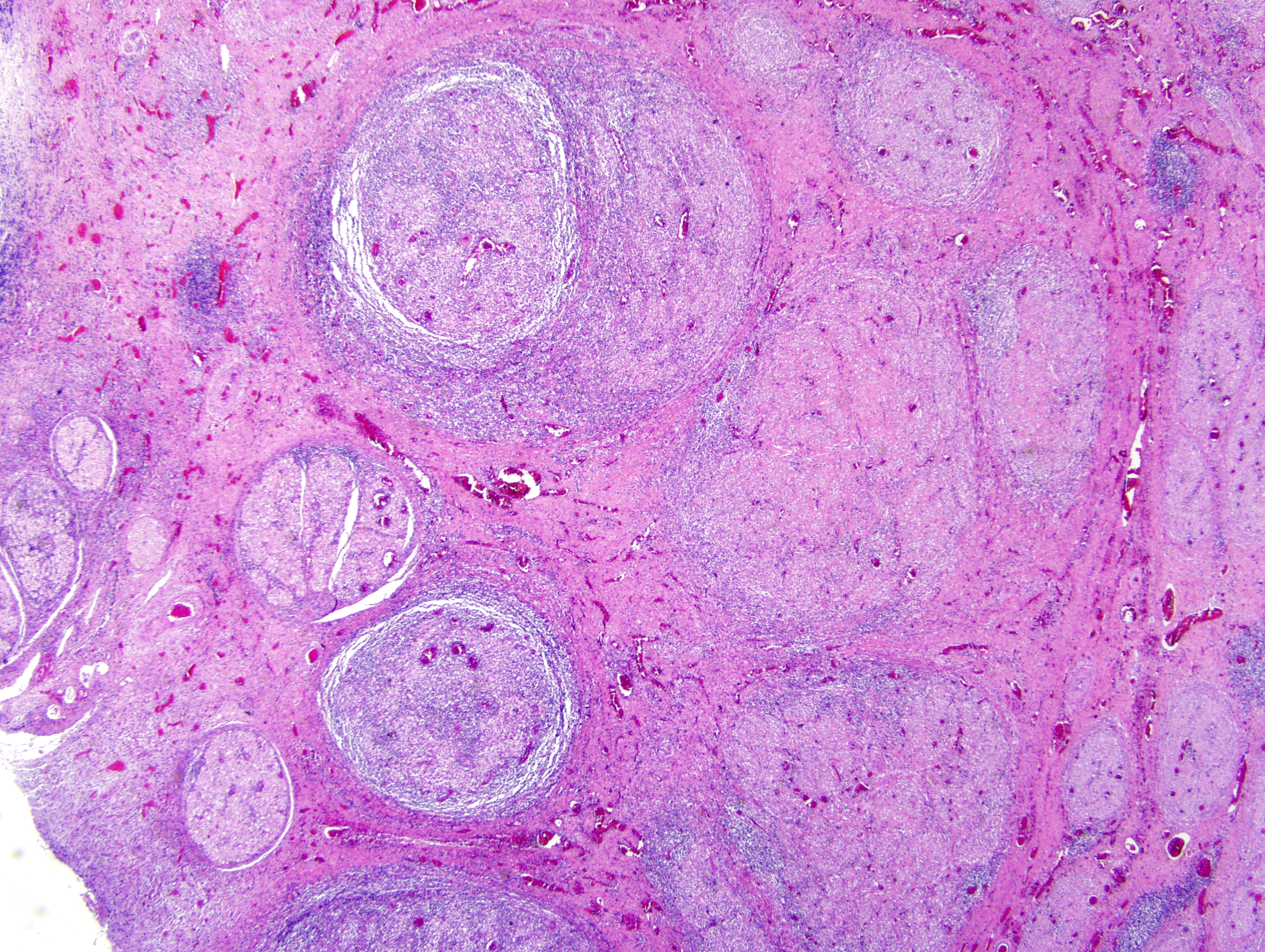
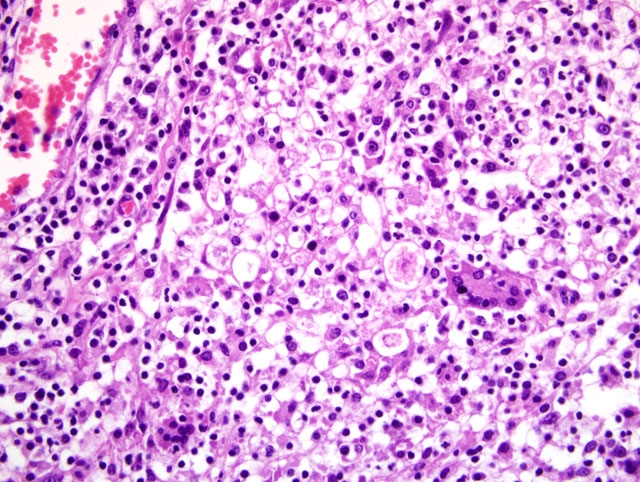
Histopathologic Description:
Cauda equina: Nerves, extradural and intradural, are moderately to severely
infiltrated by lymphocytes, plasma cells, epithelioid macrophages and fewer multinucleated giant cells. There is
axonal degeneration and loss within the affected nerves. The nerve fibers are embedded in a collagen rich fibrous
tissue (fibrosis) with a moderate lymphoplasmacytic infiltrate and focally extensive hemorrhages. Fibroplasia is
also seen within nerves. Dorsal root ganglia (not present in all sections) have a moderate to severe
lymphoplasmacytic infiltration and show axonal degeneration and loss as well as rare hypereosinophilic shrunken
neurons (neuronal necrosis). Several cranial nerves and nerves associated with hemorrhages in the gluteal region
had moderate lymphoplasmacytic infiltrates (tissue not submitted).
Morphologic Diagnosis:
Cauda equina: Neuritis and perineuritis, granulomatous, multifocal to
diffuse with epineurial and perineurial fibrosis.
Condition:
Cauda equina syndrome
Contributor Comment:
Neuritis of the cauda equina, or polyneuritis equi, is a nonsuppurative inflammation
mainly affecting the nerve trunks of the cauda equina in horses.(2) Clinically the disease is characterized by
paralysis of the tail, reduced muscle tone of the anus and rectum, paralysis of the bladder (sometimes with urinary
incontinence), paresthesia or anesthesia of the tail and perineum, and incoordination of the hindlimbs. There may
also be involvement of cranial nerves.(2) Lesions are reported to be most severe in the sacral and coccygeal nerves,
and are characterized by granulomatous inflammation, hemorrhage and fibrosis causing irregular thickening and
discoloration of the nerve roots. The inflammation is usually more severe in the extradural parts of the nerves
compared to the intradural nerve segments. Although more mildly, nerves outside the cauda equina, including
cranial nerves, are commonly also affected.(2) In the present case, nerve associated hemorrhagic lesions were
grossly visible in the gluteal region. A recent case report described biopsy of tail musculature as an aid in the
antemortem diagnosis of polyneuritis equi.(1) The cause is unknown, but the morphology of the lesion suggests that
it is an immune-mediated disorder.(2)
JPC Diagnosis:
Spinal cord, cauda equina: Polyradiculoneuritis, granulomatous, multifocally extensive, marked,
with perineural and epineural fibrosis and nerve fiber loss.
Conference Comment:
The contributor provides a succinct overview of this perplexing entity. Many favor the
term polyneuritis equi (PNE) over
neuritis of the cauda equina or
cauda equina syndrome because it more
accurately reflects the typical widespread distribution of inflammation affecting not only the cauda equina, but often
spinal roots and cranial nerves as well.(3) As alluded to by the contributor, while the pathogenesis of the lesion
remains obscure, Adenovirus I has been isolated from horses with PNE, and it is hypothesized that a viral infection
may incite an autoimmune polyradiculoneuritis in horses with this condition.(3)
Halicephalobus gingivalus has
been reported as a cause in one case of PNE.(2)
Whatever the inciting etiology, an immune-mediated mechanism is suggested by similarities with Guillain-Barre
syndrome (GBS) in humans and experimental allergic neuritis (EAN) in laboratory animals. Specifically, PNE,
GBS and EAN are all characterized by demyelination in the proximal roots with invading mononuclear cells and
macrophages stripping away segments of the myelin sheath. Furthermore, circulating antibodies to the P2 myelin
protein, the antigen that upon injection into laboratory animals produces EAN, have been demonstrated in horses
with PNE. Nevertheless, the role of these antibodies in the pathogenesis of PNE is unknown; they may be causal or
arise secondary to demyelination and inflammation.(3)
As mentioned by the contributor, a recent case report describes biopsy of the sacrocaudalis dorsalis lateralis muscle,
the innervation of which arises in the cauda equina, for the antemortem diagnosis of PNE. In frozen biopsy
specimens, intense lymphohistiocytic inflammation infiltrated and effaced terminal intramuscular nerve branches
while sparing the myofibers, which exhibited angular atrophy of both muscle fiber types (neurogenic atrophy) and
occasional hypertrophic or split fibers.(1)
References:
1. Aleman M, Katzman SA, Vaughan B, Hodges J, Crabbs TA, Christopher MM, Shelton GD, Higgins RJ:
Antemortem diagnosis of polyneuritis equi. J Vet Intern Med
23:665-668, 2009
2. Maxie MG, Youssef S: Nervous system.
In: Jubb, Kennedy, and Palmers Pathology of Domestic Animals, ed.
Maxie MG, 5th ed., vol. 3, p. 444. Elsevier Saunders, Philadelphia, PA, 2007
3. Summers BA, Cummings JF, De Lahunta A: Veterinary Neuropathology, pp. 433-434. Mosby, St. Louis, MO,
1995