Signalment:
Two-year-old, male, Weimaraner,
Canis familiaris The patient had a chronic vomiting problem of one-year duration. The dog was thin with atrophy of all muscles except those of the neck and tongue. Radiographs showed a hiatal hernia. The tongue was difficult to exteriorize for anesthesia due to a large sublingual mass. Front limbs became spastic during anesthesia. Electromyogram demonstrated spontaneous activity, complex repetitive activity, and high frequency discharges, but motor nerve conduction velocities were normal. Myoglobinuria was noted. Due to the clinical diagnosis, this dog was euthanized.
Gross Description:
The dog had left side abdominal cryptorchidism and right side renal agenesis. A left side esophageal hiatal hernia contained the stomach and duodenum. Most importantly, the dog had massive thickening of the muscles of the base of the tongue, and that musculature pulled the mandible caudally. The tongue was short and triangular with a base 10cm in diameter (the mass noted clinically). The neck muscles were thick, giving a buffalo hump appearance. The diaphragmatic muscle surrounding the central tendon was pale and 1.5cm thick; however, overall short. The body muscle mass was reduced and muscles were pale.
Histopathologic Description:
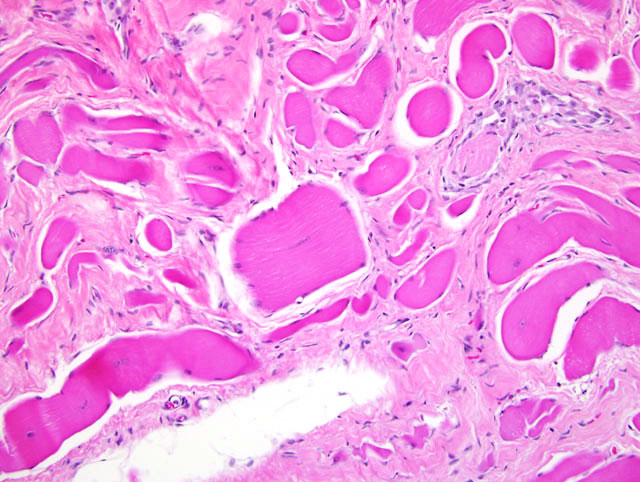
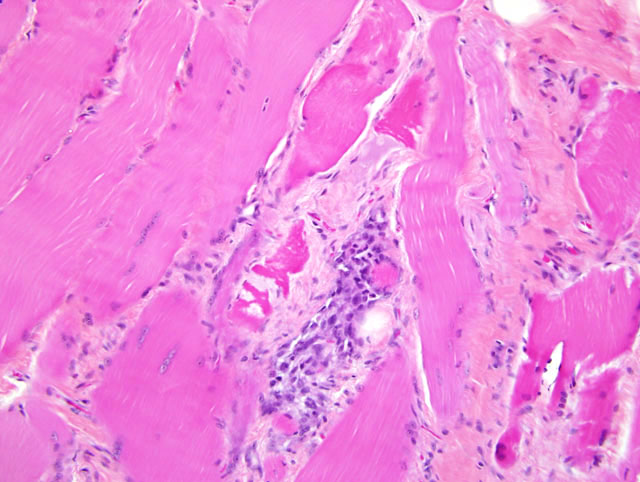
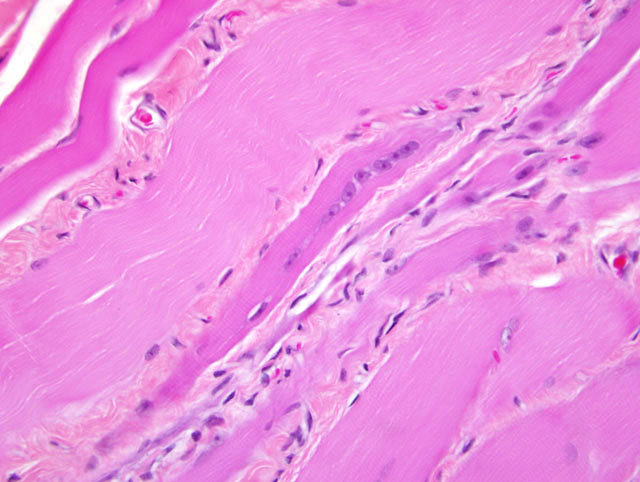
The slide presented is of the diaphragm of the patient and a normal size and age-matched dog. On subgross, one notes the obvious and impressive difference in thickness of the longintudinal sections. The thickness is attributed to fibrosis, degenerating hypercontracted, hyelinized, broken and thick fibers with central fiber cysts and nuclei within fibers, as well as on-going regeneration and hypertrophy with proliferation of satellite muscle. The resident fat of the diaphragm remains. Mineralization is present.Â
Morphologic Diagnosis:
Diaphragm Severe, diffuse, myodegeneration and necrosis with mineralization and fibrosis and on-going myoregeneration (muscular dystrophy).Â
Lab Results:
Creatinine Kinase 32672 u/L (reference range 68 400 u/L); Serum Alanine Aminotransferase 305 u/L (reference range 10 130 u/L); WBC 21,500 cells/u/L (reference range 6,000 17,000) with an absolute neutrophilia of 18,050 cells / u/L.
Condition:
Dystrophin-deficient muscular dystrophy
Contributor Comment:
The lesions are typical of the muscular dystrophy described in Golden Retrievers.
6,7,8 Immunostaining for dystrophin showed absence of dystrophin (a membrane-associated protein) below the membranes of muscle fibers from the sublingual area, sternohyoideous, and infraspinatus. Thus, this case represents another breed with Duchenne-like muscular dystrophy. Similar X-linked muscular dystrophy has been demonstrated in Golden Retrievers, Labrador Retrievers, Irish Terriers, Samoyeds, Rottweillers and the Japanese Spitz.
1,5 Affected animals lack the subsarcolerminal protein, dystrophin. Clinically, they show progressive weakness and later cardiac abnormalities. This dog also had a dilated and hypertrophic myocardium with severe cardiomyopathy. The unusual presenting clinical complaint, chronic vomiting, is presumed due to the hiatal hernia. Interestingly, Duchenne-like muscular dystrophy researchers using Golden Retrievers found a left side hiatal hernia in their breeding colony.
9 Difficiency of the 427 KD dystrophin protein has been demonstrated in humans, cats, dogs and mice.
2,3,4,7
The obvious difference in thickness of the longitudinal sections is attributed to hypercontracted, hyalinized, broken, swollen fibers, some having central cysts and central nuclei. These fibers are often separated by extensive fibrosis. Some fiber hypertrophy with sarcolemmal nuclei proliferation is ongoing.
JPC Diagnosis:
Skeletal muscle: Myocyte hypertrophy,
degeneration, necrosis, regeneration, and mineralization,
diffuse, severe, with fibrosis, Weimaraner, (
Canis
familiaris), canine
(fig. 3-1, 3-2, 3-3).
Conference Comment:
X-linked muscular dystrophy,
an X-linked recessive defect in the dystrophin gene, affects
approximately 50% of males born to female carriers.
10 The dystrophin gene codes for a membraneassociated
cytoskeletal protein that is present in skeletal
and cardiac muscle. The lack of this gene increases the
susceptibility of the muscle fibers to repeated bouts of
necrosis, regeneration, and fibrosis.
10 Dystrophin deficiency
generally results in progressive muscle atrophy of
most breeds of dogs, but may cause marked muscle hypertrophy
in cats, mice, and Rat Terrier dogs.
3,11
Characteristic gross pathological findings include severe
degeneration of the diaphragm and strap muscles with
pale white streaks within the affected muscles.
11
Not all canine muscular dystrophies are X-linked. A defect
in sarcoglycan, a component of the sarcolemmal dystrophin
glycoprotein complex, occurs in both male and
female dogs.
10
Negative immunohistochemistry for the dystrophin protein
is helpful in diagnosing muscular dystrophy, although
a positive result will not rule out the entity. Partial
expression of dystrophin may occur in Becker-type
mutations or in revertant fibers, in which genetic mutation
allows some dystrophin expression.
11
References:
1. Bergman RL, Inzana KD, Monroe WE, Shell LG, Liu LA, Engvall E, Shelton GD: Dystrophin-deficient muscular dystrophy in a Labrador retriever. J Am Anim Hosp Assoc 38:255-261, 2002
2. Collins CA, Morgan JE: Duchennes muscular dystrophy:
Animal models used to investigate pathogenesis and diagnosdevelop
therapeutic strategies. Int J Exp Pathol 84:165-172, 2003
3. Gaschen FP, Hoffman EP, Gorospe JRM, Uhl EW, Senior DF, Cardinet III GH, Pearce LK: Dystrophin deficiency causes lethal muscle hypertrophy in cats. J Neurol Sci 110:149-159, 1992
4. Gaschen L, Lang J, Lin S, Ade-Damilano M, Busato A, Lombard CW, Gaschen FP: Cardiomyopathy in dystrophin-deficient hypertrophic feline muscular dystrophy. J Vet Intern Med 13:346-356, 1999
5. Jones BR, Brennan S, Mooney CT, Callanan JJ, McAllister H, Guo LT, Martin PT, Engvall E, Shelton GD: Muscular dystrophy with truncated dystrophin in a family of Japanese spitz dogs. J Neurol Sci 217:143-149, 2004
6. Valentine BA, Cooper BJ, Cummings JF, deLahunta A: Progressive muscular dystrophy in a golden retriever dog: light microscope and ultrastructural features at 4 and 8 months. Acta Neuropathol (Berl) 71:301-310, 1986
7. Valentine BA, Cooper BJ, Cummings JF, deLahunta A: Canine X-linked muscular dystrophy: morphologic lesions. J Neurol Sci 97:1-23,1990
8. Valentine BA, Cooper BJ, Dietze AE, Noden DM: Canine congenital diaphragmatic hernia. J Vet Intern Med 2:109-112, 1988
9. Valentine BA, Winand J, Pradhan D, Moise NS, deLahunta A, Korneygay JN, Cooper BJ: Canine X-linked muscular dystrophy as an animal model of Duchenne muscular dystrophy: a review. Am J Med Genet 42:352-356, 1992
10. Valentine BA, McGavin: Skeletal muscle. In: Pathologic
Basis of Veterinary Disease, eds. McGavin MD,
Zachary JF, 4th ed., pp. 1026-1029, 1035-1037. Elsevier,
St. Louis, MO, 2007
11. Van Vleet JF, Valentine BA: Muscle and tendon. In:
Jubb, Kennedy, and Palmers Pathology of Domestic
Animals. ed. Maxie MG, 5th ed., vol. 1, pp. 210-216.
Saunders Elsevier, Endinburgh, 2007