Results
AFIP Wednesday Slide Conference - No. 9
3 November 1999
-
- Conference Moderator:
Dr. John Pletcher, Diplomate, ACVP
Pathology Associates International
15 Worman's Mill Court
Frederick, MD 21701
-
- NOTE: Click on images for larger views. Use
browser's "Back" button to return to this page.
Return to WSC Case Menu
-
- Case I 98-0712 (AFIP# 2677999)
-
- Signalment: Six-month-old CD1xC57Bl/6 female mouse.
-
- History: This female mouse presented with a severely
distended abdomen. The investigators suspected she might have
hepatic pathology (tumor, cirrhosis, or necrosis) and ascites,
because this strain of mouse carries a null allele in the DcoH
gene, a gene of some importance in liver function. The mouse
was euthanized with CO2 and necropsied.
-
- Gross Pathology: The only lesion was a markedly enlarged
left kidney. The kidney consisted of a balloon-like structure
with a transparent renal capsule, measured 4 x 2.5 x 2 cm., and
was filled with slightly turbid yellow-orange fluid. A .9 x .7
x .7 cm pale tan, irregular sessile mass protruded into the lumen
from the area identified as the renal pelvis.
-
 A
A B
B C
C
- Case 9-1. A) Distended abdomen. B) Within the left
upper quadrant there is a 2.5x3.5cm cystic brown-pink mass. C)
The left kidney is replaced by a (now ruptured) thin walled cystic
structure with a multilobular, sessile, white mass extending
from the wall.
-
- Laboratory Results:
A direct Gram stain of the fluid from the kidney revealed no
bacteria, and 4+ large amorphous crystals. There was no aerobic
growth after 5 days.
- Contributor's Diagnoses and Comments: Left kidney, pelvis:
Carcinoma, transitional cell (primary differential), with glandular
metaplasia.
Severe hydronephrosis and marked chronic active pyelitis.
-
- Located within the renal pelvis, an irregular sessile, somewhat
papillary mass projects into the large cystic space in this severely
hydronephrotic kidney. The mass is incompletely covered by bilayered
to pseudostratified, relatively well differentiated cuboidal
epithelium (transitional epithelium), yet there is extensive
down growth and stromal invasion by poorly differentiated epithelial
cells forming nests, gland-like, and pseudo-tubular structures
within the body of the mass. There is mild to moderate nuclear
pleomorphism and a low mitotic index. The variably dense fibrous
stroma contains high numbers of inflammatory cells including
neutrophils, plasma cells (some with Russell bodies), eosinophils,
lymphocytes and hemosiderin-laden macrophages. The remaining
renal parenchyma has been reduced to a thin shell of dense fibrous
connective tissue, rare sclerotic glomeruli and moderate numbers
of mixed inflammatory cells.
-
- Primary renal neoplasias in mice represent less than 1% of
spontaneously arising tumors. Spontaneous tumors of the renal
pelvis are extremely rare. Transitional cell carcinomas of the
renal pelvis, when extremely invasive and poorly differentiated,
may be difficult to distinguish from renal cell carcinomas. In
the mouse, urinary bladder pathology induced by certain compounds
such as 4-ethylsulfonylnaphthalene-1-sulfonamide (ENS) and Benzidine
may result in a range of morphologic diagnoses for the same lesion,
including chronic cystitis, papillary hyperplasia, or noninvasive
carcinoma, whereas 2-Acetylaminofluorene (2-AAF), is more commonly
associated with the induction of renal adenomas and carcinomas,
as well as carcinomas of the urinary bladder. In all studies,
mice developing lesions are considerably older (1-2 yrs) than
the mouse in this case (6 months). The presence of this large
mass in the renal pelvis gradually obstructed urinary outflow,
resulting in an extreme case of hydronephrosis and the very distended
abdomen seen clinically (see gross photographs).
-
- AFIP Diagnosis: Renal pelvis: Transitional cell carcinoma,
with hydronephrosis and chronic-active inflammation, CD1xC57Bl/6
mouse, rodent.
-
- Conference Note: Very few slides contain any remaining
renal tissue, due to this fact most conference participants preferred
a differential diagnosis of Transitional cell carcinoma, ovarian
carcinoma, or renal cell carcinoma.
Although spontaneous neoplasia of the renal pelvis is extremely
rare in mice, its characteristics of malignancy and biologic
behavior are generally the same as those affecting the urinary
bladder. These tumors are generally papillary, variably invasive,
with pleomorphic to anaplastic cells and commonly demonstrate
varying degrees of squamous metaplasia.
-
- Contributor: Department of Comparative Medicine, Stanford
University School of Medicine, Quad 7, Bldg 330, Stanford, CA
94305-5410
-
- References:
- 1. Boorman GA, Wood M, Fukushima S: Tumours of the urinary
bladder. In: Pathology of Tumours in Laboratory Animals, Vol.
II, Tumours of the Mouse. pp. 383-406. IARC, France, 1994
- 2. Frith CH, Terracini B, Turusov VS. Tumors of the kidney,
renal pelvis and ureter. In: Pathology of Tumours in Laboratory
Animals Vol. II Tumours of the Mouse, pp. 357-381. IARC, France,
1994
- 3. Frith CH, Farmer JH, Greenman DL: Biologic and morphologic
characteristics of urinary bladder neoplasms induced in BALB/c
female mice with 2-acetylaminofluorene. Journ of Enviro Pathol
and Tox, 3:103-119, 1979
- 4. Frith CH: Report of a workshop on urothelial lesions in
mice. Journ of Enviro Pathol and Tox, 1:617-626, 1978
- 5. Shinohara Y, Frith CH: Morphologic characteristics of
benign and malignant renal cell tumors in control and 2-Acetylaminofluorene-treated
BALB/c female mice. Amer Journ of Pathol, 100:455-468, 1980
-
-
- Case II Case 1 (AFIP 2505896)
-
- Signalment: 54-week-old female CD-1 VAF mouse.
-
- History: This control mouse was killed in extremis
during week 48 of a two-year carcinogenicity study. It was housed
in an environmentally controlled room and was fed a certified
rodent chow ad libitum.
-
- Gross Pathology: The liver was enlarged and contained
multiple raised 0.5-1.0 cm diameter nodules in all lobes. The
uterus contained a tan 1.0-2.0 cm diameter mass in the left uterine
horn.
-
- Contributor's Diagnoses and Comments: Liver: Histiocytic
sarcoma.
-
- Diffusely, liver sinusoids are infiltrated by round to fusiform
neoplastic cells that randomly from irregular sheets and efface
the parenchyma. Cells have large round to oval nuclei and abundant
eosinophilic cytoplasm. Similar neoplastic proliferations were
present in the uterus, cervix, bone marrow, skin (ventral abdomen),
lung, mesenteric lymph node, right adrenal, meningeal vessels,
colonic serosa, and mesenteric fat.
-
- This neoplasm has also been referred to as reticulum cell
sarcoma type A, malignant lymphoma (histiocytic type), histiocytic
lymphoma, endometrial sarcoma, and malignant schwannoma. Research
indicates that the cells are derived from histiocytes. Cells
are positive for lysozyme, a-1 antitrypsin, Mac-2, and less commonly
c-FMS. Histiocytic sarcomas are rare before 12 months of age,
and are more common in females.
-
- The liver is the most commonly affected organ in males and
the uterus, vagina, and/or liver are often primary sites in females.
Other organs that may be affected include spleen, lymph node,
bone marrow, lung, kidney and ovaries. Metastasis to the lung
is common when there is liver involvement.
-
- AFIP Diagnosis: Liver: Histiocytic sarcoma, CD-1 VAF
mouse, rodent.
-
- Conference Note: Histiocytic sarcomas (HS) are common,
highly malignant tumors in mice with an incidence of up to 22%
percent in certain strains. HS are uncommon in mice younger than
one year of age, and have been associated with viral etiologies.
HS may be accompanied by myeloid hyperplasia in the spleen, and
in some strains by hyaline droplets (accumulations of lysozyme-containing
organelles) in the renal proximal tubular epithelium.
-
- Contributor: Wyeth-Ayerst Research, 42 Ayerst Lab
Rd., Chazy, NY 12921
-
- References:
- 1. Faccini JM, DP Abbott, Pautus GJJ: Hematopoietic and lymphatic
systems. In: Mouse Histopathology, a glossary for use in toxicity
and carcinogenicity studies, pp. 18-36. Elsevier, New York, 1990
- 2. Frith CH, PK Pattengasole, Ward JM: Neoplastic lesions.
In: A Color Atlas of Hematopoietic Pathology of Mice, pp. 7-13.
Toxicology Pathology Associates Little Rock, Arkansas, 1985
- 3. Frith CH, JM Ward, Chandra M: The morphology, immunohistochemistry
and incidence of hematopoietic neoplasms in mice and rats. Tox
Path 21(2):206-218, 1993
- 4. Ward JM, Sheldon W: Expression of mononuclear phagocyte
antigens in histocytic sarcoma of mice. Vet Pathol 30:560-565,
1993
-
-
- Case III NIAH (AFIP# 2681359)
-
- Signalment: A three-month-old, male, dog
-
- History: The dog was vaccinated at one month of age
(the type of vaccine is unknown). The dog showed depression,
coughing, tremor, eye and mucus. It was euthanized.
-
- Gross Pathology: The subcutaneous and abdominal fat
was decreased. There was a small amount of serosanguinous pleural
effusion. The lungs were congested and its cut surface edematous.
The thymus was severely atrophied.
-
- Laboratory Results: No biochemical examination was
performed. A spleen emulsion from the affected dog was injected
into a normal dog, which subsequently developed fever and leukopenia.
Isolation of canine distemper virus was unsuccessful.
Contributor's Diagnosis and Comments: Lung, pneumonia,
interstitial, with intranuclear inclusion bodies and intracytoplasmic
inclusion bodies, dog.
-
- Etiology: Canine adenovirus-2 and canine distemper
virus
-
- In the lung, eosinophilic or basophilic intranuclear inclusion
bodies were found in alveolar epithelial cells, alveolar macrophages,
and bronchial epithelial cells. In some areas, congestion, hemorrhage,
edema and infiltration of neutrophils, macrophages, lymphocytes,
and plasma cells were noted, which suggested a secondary bacterial
infection. Intranuclear inclusion bodies were also found in epithelial
cells of gallbladder, renal tubules, pancreatic ductules and
gastrointestinal tract, as well as in adrenal cortical cells
and lymph node follicular dendritic cells. Immunohistochemical
staining with anti-canine adenovirus-2 monoclonal antibody showed
a positive reaction in some inclusion bodies.
In addition, eosinophilic intracytoplasmic inclusion bodies were
found in bronchial epithelial cells, but immunohistochemical
staining for canine distemper virus antigen failed to produce
a positive reaction. However, electron microscopic examination
revealed the typical ultrastructure of canine distemper virus-type
particles as well as adenovirus particles.
This case was deduced to be a mixed infection with canine distemper
virus and canine adenovirus-2. It demonstrates the importance
of careful examination for infectious agents.
-
- AFIP Diagnosis: Lung: Bronchopneumonia, proliferative
and necrotizing, subacute, diffuse, moderate, with large basophilic
and eosinophilic intranuclear inclusion bodies and small eosinophilic
intracytoplasmic inclusion bodies, breed unspecified, canine,
etiologies consistent with canine adenovirus-2 and canine distemper
virus.
-
- Conference Note: Conference participants agreed with
the contributor's assessment. Large, eosinophilic to basophilic
intranuclear inclusion bodies typical of canine adenovirus infection,
and small, eosinophilic intranuclear and intracytoplasmic inclusion
bodies consistent with those seen in cases of canine distemper
are present. Small numbers of syncytial cells characteristic
of canine distemper were also observed.
-
- Pneumonias caused by canine adenovirus are most commonly
found in conjunction with canine distemper virus infection or
other conditions resulting in immune suppression.
Contributor: National Institute of Animal Health, Kannondai
3-1-1, Tsukuba, Ibaraki 305-0856, Japan
-
- References:
- Dungworth DL: The Respiratory System. In: Pathology of Domestic
Animals, vol. 2, eds. Jubb KVF, Kennedy PC, Palmer N, 4th ed.
pp. 617-627. Academic Press, San Diego, CA, 1993
-
-
- Case IV - 11142-98 (AFIP 2679507)
-
- Signalment: Beaver (Castor canadensis), adult female,
35-pounds.
-
- History: This beaver was one of six that died within
a 2-week span in a southern Indiana wildlife reserve.
-
- Gross Pathology: Fibrin-containing fluid filled the
pleural and peritoneal cavities. Fibrin covered the pulmonary
pleura, diaphragmatic peritoneum, and the capsules of the liver
and spleen. White-yellow foci were widely disseminated throughout
the liver and spleen. Similar foci were dispersed along the dilated
and yellow-white mesenteric lymphatic vessels. Mesenteric lymph
nodes were enlarged and firm. On section, they consisted mostly
of friable, yellow-white areas. Within the uterus were three
near-term fetuses. Placentas and the endometrium were dark red
and edematous with scattered yellow-white foci.
-
 A
A B
B
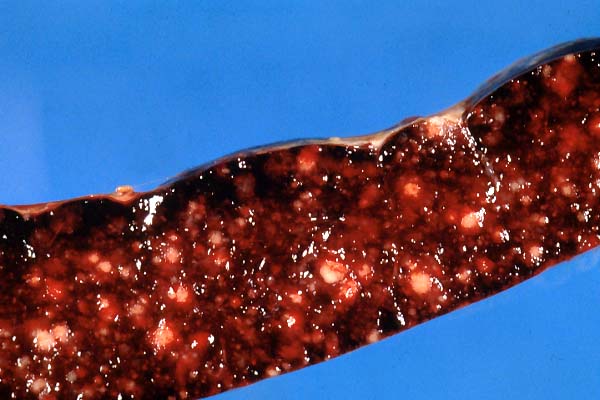
- Case 9-4. A) There are diffusely distributed variably
sized white to tan (necrotic) foci replacing hepatic parenchyma.
B) On cut section, the spleen contains multiple variably sized
2-5mm (necrotic) foci.
-
- Laboratory Results: Francisella tularensis subsp.
palaearctica (Type B) was isolated from the liver and spleen.
Contributor's Diagnoses and Comments:
- 1. Liver: Hepatitis, necrotizing (necrosuppurative), acute,
multifocal, with thromboangiitis.
2. Spleen: Splenitis, necrotizing (necrosuppurative), acute,
multifocal, with thromboangiitis.
-
- This case is an example of tularemia in a beaver. Inflammation
typical of tularemia was also identified in the placenta and
mesenteric lymph nodes and lymphatic vessels. Type B Francisella
tularensis (Francisella tularensis subsp. palaearctica) is distributed
worldwide and primarily occurs in water-dwelling rodents. Type
A Francisella tularensis (Francisella tularensis subsp. tularensis)
is mostly limited to North America and infects rabbits and occasionally
humans. Tularemia has also been reported in cats. Infection can
be acquired directly or through vectors (e.g., tick or deerfly).
-
- AFIP Diagnosis: Liver and spleen: Hepatitis and splenitis,
necrotizing, acute, multifocal, moderate, with multifocal necrotizing
vasculitis.
-
- Conference Note: Tularemia is endemic worldwide, primarily
causing disease in rodents and lagomorphs. Dermacentor and Amblyoma
ticks pass the organism transstadially and transovarially, functioning
as both vectors and reservoirs. Mosquitoes, fleas, horseflies,
and lice can also transmit the disease, and there are numerous
reports of zoonotic infections resulting from dog and cat bites.
Carnivores may be infected by ingesting infected carcasses.
F. tularensis is a small, pleomorphic, heat-labile, gram-negative,
facultative intracellular coccobacillus that is surrounded by
a thick, lipid-rich capsule. All isolates are antigenically similar,
but they are subdivided, based on virulence, epidemiological,
and biochemical characteristics into three subspecies or biovars:
1. ssp. tularensis (Type A): most virulent; found in North America;
associated with tick-borne tularemia in rabbits and zoonotic
disease.
2. ssp. palaearctica (Type B): less virulent; found worldwide
except for Australia and Antarctica; associated with waterborne
disease of rodents.
3. ssp. mediasiatica: found in central Russia.
-
- The organism usually enters the host via inoculation by arthropods,
skin abrasions, or mucous membranes of the eye or oronasopharynx.
It is generally accepted that the organisms are taken up by local
macrophages. Intrahistiocytic replication occurs in local lymph
nodes. Septicemia develops after 3-14 days, disseminating organisms
to the spleen, liver, lymph nodes and bone marrow and causing
the consistent necropsy finding of numerous small white foci
on the surface of the liver, spleen (as depicted in the gross
color transparencies submitted with this case), lymph nodes,
and, less often, kidneys. In acute septicemia, an initial neutrophilia
is often followed by neutropenia.
-
- Disease susceptibility varies with species infected. Rodents
and lagomorphs are most susceptible, and usually suffer fatal
septicemia. Other herbivores, ruminants and birds are susceptible,
but mortality is unusual. Carnivores are least susceptible, and
require a large infective dose, rarely develop bacteremia, and
only occasionally manifest overt disease. Differential diagnosis
considered in this case included infections caused by Clostridium
piliforme, Salmonella spp., Listeria monocytogenes, Toxoplasma
gondii, and Yersinia spp.
-
- Francisella tularensis can be grown in culture, but the potential
risk of human infection requires extra caution. The preferred
diagnostic test is serology. A four-fold rise in antibody titer
between acute and convalescent serum is considered diagnostic;
however, cross-reaction with Brucella antigen can occur. IFA
is available. Organisms are visible on smears stained with new
methylene blue.
-
- Contributor: Animal Disease Diagnostic Laboratory,
ADDL-1175, Purdue University, West Lafayette, IN 47907
-
- References:
- 1. Davidson WR, Nettles VF:. Beaver (Castor canadensis).
In: Field Manual of Wildlife Diseases in the Southeastern United
States. 2nd ed., pp. 230-231. Southeastern Cooperative Wildlife
Disease Study. Athens, GA, 1997
- 2. Davidson WR, Nettles VF: Tularemia. In: Field Manual of
Wildlife Diseases in the Southeastern United States. 2nd ed.,
pp. 235-238. Southeastern Cooperative Wildlife Disease Study.
Athens, GA, 1997
- 3. Gliatto JM, Rae JF, McDonough PL, Dasbach JJ: Feline tularemia
on Nantucket Island, Massachusetts. J Vet Diagn Invest 6:102-105,1994
- 4. Rohrbach BW: Tularemia. In: Zoonosis Updates. J Am Vet
Med Assoc. Schaumburg, IL, 1990
- 5. Woods JP, Panciera RJ, Morton RJ, Lehenbauer TW: Feline
tularemia. Compendium 20(4):442-457, 1998
- 6. Woods JP, Crystal MA, Morton RJ, Panciera RJ: Tularemia
in two cats. J Am Vet Med Assoc 212(1):81-83, 1998
-
-
- J Scot Estep, DVM
Captain, VC, USA
Registry of Veterinary Pathology*
Department of Veterinary Pathology
Armed Forces Institute of Pathology
(202)782-2615; DSN: 662-2615
Internet: estep@afip.osd.mil
-
- * The American Veterinary Medical Association and the American
College of Veterinary Pathologists are co-sponsors of the Registry
of Veterinary Pathology. The C.L. Davis Foundation also provides
substantial support for the Registry.
-
- Return to WSC Case Menu
 A
A B
B C
C