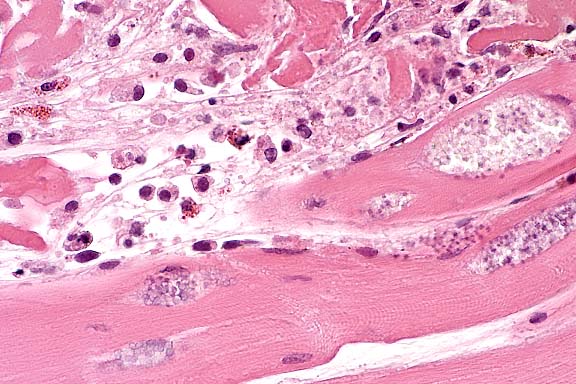
(Microsporidia) separate viable muscle fibers. Scattered lymphocytes, heterophils, and histiocytes expand the interstitium.
40X
Signalment: Adult, female, pancake tortoise (Malacochersus tornieri)
History: This adult tortoise was noted to be lethargic and anorectic. Radiographs taken 2 weeks after the onset of clinical signs revealed the presence of a large egg within the caudal abdomen. The tortoise was administered an intramuscular injection of calcium gluconate and returned to its exhibit. Clinical signs did not improve. It was found dead approximately 6 weeks after the onset of clinical signs.
Gross Pathology: The tortoise was in poor nutritional condition and moderately dehydrated. Skeletal musculature was atrophic and contained numerous pale tan to white streaks. Approximately 30 ml of clear yellow fluid was present in the coelomic cavity. A large fully-shelled egg was located in the left oviduct. There were no other significant gross findings.
Laboratory Results: Hematologic and plasma chemistry results from a blood sample collected 4 weeks prior to death were unremarkable.
Contributor's Diagnosis and Comments: Skeletal muscle; myositis, acute to chronic, multifocal, moderate, with protozoa. Etiology: microsporidia
This tortoise had multifocal myofiber degeneration and necrosis accompanied by inflammation which affected skeletal muscles throughout the body. These lesions varied from acute to chronic and were associated with the presence of numerous oval 1-1.5 X 2.5-3 mm organisms located within sarcoplasm and extracellularly. These organisms could also occasionally be found within non-degenerate myofibers near the inflammatory foci. The organisms were gram positive, acid-fast, and contained single PAS-positive polar granules. The morphology and staining characteristics are typical of microsporidian protozoa.
Other significant lesions in this animal were limited to splenic lymphoid depletion and generalized atrophy of body fat. The myositis was severe enough to have interfered with this tortoise's ability to move resulting in the lethargy and anorexia noted clinically, and ultimately the animal's death.
Several species of microsporidia have been reported in invertebrate animals, fish and amphibians. Encephalitozoon cuniculi may infect a wide variety of mammals and other microsporidia have recently been discovered in immunocompromised humans. However, there are few reports of microsporidial infections in reptiles; species affected include tuataras (Sphenodon punctatus), the European common wall lizard (Podarcis muralis), inland bearded dragons (Pogona vitticeps), the European grass snake (Natrix natrix), the split keelback snake (Atretium schistosum), and a garter snake (Thamnophis sp.). There appears to have been one previous report of an infection in a chelonian, the European swamp turtle (Emys orbicularis), but it is unclear whether there was any clinical disease or lesions associated with this.
Conference Note: Members of the phylum Microspora are all obligate intracellular parasites that form spores. Well-known examples include Encephalitozoon cuniculi, a frequent pathogen of rodents and rabbits; Nosema apis, a major killer of bees; and Nosema bombycis, the cause of silkworm disease, which caused devastation of the silk industry in Europe in the nineteenth century.7
The three major components of the microsporidian spore are
the spore wall, sporoplasm, and an extrusion apparatus. The extrusion
apparatus consists of a polar filament, which is coiled in an
inverted position inside the spore and is formed by a special
Golgi apparatus, the posterosome. Upon contact of the spore with
the host cell, the distal end of the polar filament uncoils and
penetrates the cell. The sporoplasm is then squeezed through the
narrow, hollow tube of the filament.1,7,8 All active stages of
the parasite develop in the cytoplasm of the host cell.
Contributor: National Zoological Park, Smithsonian Institution,
Washington, D.C. 20008
International Veterinary Pathology Slide Bank:
Laser disc frame #24378
Signalment: Approximately 8-year-old, male, San Lucan speckled rattlesnake (Crotalus mitchelli).
History: Found dead with no premonitory signs.
Gross Pathology: The trachea contained abundant thick
pale tan/yellow mucoid exudate that was mixed with blood caudally.
Similar exudate partially filled the lumen of the cranial lung.
The caudal lung contained clots and strands of blood. Lung parenchyma
was moist and red.
Laboratory Results: Escherichia coli was cultured from
a swab of the lung. Paramyxovirus was isolated from lung tissue
by Dr. Melissa Kennedy, University of Tennessee.
Etiology: paramyxovirus and secondary Escherichia coli.
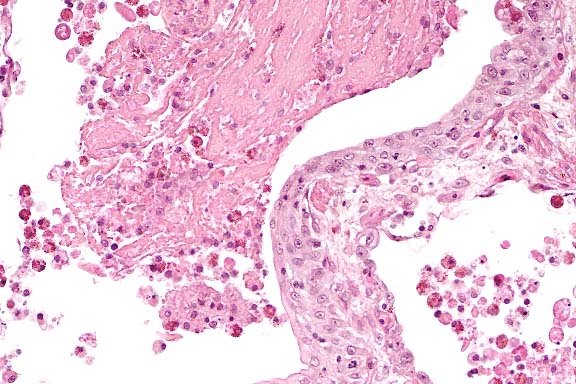
Conference Note: Gram stains performed at the AFIP demonstrated many gram-negative bacilli within the exudate in the tracheal lumen.
Conference participants observed multinucleated giant cells within the pancreas, but were unable to definitively characterize them based on histomorphology alone. Although these may represent virus-induced syncytial cells, the possibility that they are histiocytic giant cells cannot be excluded.
There are presently four genera within the family Paramyxoviridae, i.e. Rubulavirus, Paramyxovirus, Morbillivirus, and Pneumovirus. Genetic characteristics of the ophidian paramyxoviruses are significantly different than any of the currently described genera, and warrant an additional genus to be named within the Paramyxoviridae (D. Nichols, personal communication). The relative degree of susceptibility of snakes to paramyxoviral disease is Viperidae>Elapidae>Colubridae>Boidae (D. Nichols, personal communication).
Contributor: Zoological Society of San Diego, P.O. Box 551, San Diego, CA 92112-0551
International Veterinary Pathology Slide Bank:
Laser disc frame #11300, 11303, 11325, 11390
Signalment: 17-day-old, female, emerald starling (Lamprotornis iris).
History: This was a recently fledged bird, found dead on the ground.
Gross Pathology: There was marked pulmonary edema and hepatosplenomegaly.
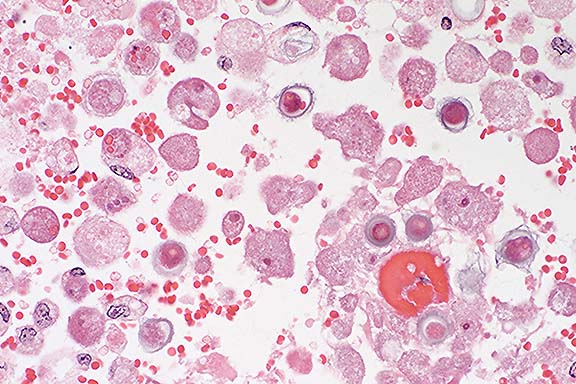
Contributor's Diagnosis and Comments: Pneumonia, lymphohistiocytic, diffuse, severe (sludging of leukocytes in blood vessels), with intraleukocytic protozoal zoites.
Etiology: Atoxoplasma sp.
Although we have called this a pneumonia (to facilitate coding and retrieval), the lesion most likely represents sludging of leukocytes in pulmonary capillaries, rather than a true pneumonia. Larger blood vessels are also packed with leukocytes containing protozoal zoites.
The differential diagnosis in this case would include Sarcocystis sp., Toxoplasma gondii, Haemoproteus sp., Histoplasma sp., and Candida sp. infection. Sarcocystis sp. and Haemoproteus sp. can be ruled out because of the lack of sinuous schizonts in capillaries. Toxoplasma gondii can be ruled out because of the size of the zoites and number of zoites per cell. Special stains have ruled out Histoplasma sp. and Candida sp.
This bird also had marked intestinal coccidiosis, which may represent the sexual stage of the infection.
Conference Note: Atoxoplasma spp. are single-host, species-specific coccidia affecting passerine birds. Transmission is direct via oocysts deposited in feces. Infection begins with ingestion of sporulated oocysts, with each oocyst containing two sporocysts that further contain four sporozoites. Sporozoites are released in the intestinal lumen, then invade epithelial cells, lymphocytes, and macrophages and are then disseminated throughout the tissues of the body. Merogony occurs in mononuclear cells in the blood and in intestinal epithelium. Gametogeny occurs in the intestinal epithelial cells of the same individual. Oocysts sporulate outside the host.
Gross lesions of atoxoplasmosis may include hepatomegaly with multiple pinpoint white foci covering the surface and throughout the parenchyma; similar white foci in the pericardium and myocardium; splenomegaly; and effusion in pericardial and air sacs.1 Although the organism is often difficult to see in H&E-stained histologic sections, it is much easier to detect by cytological examination of Wright's-stained impression smears of liver.
Contributor: Zoological Society of San Diego, P.O. Box 551, San Diego, CA 92112
Signalment: 4-year-old Montdale ram.
History: Posterior paralysis beginning 8 days prior to death. Progression of clinical signs resulted in recumbency and blindness, with diminished level of consciousness. Temperature 1 day prior to death was 107.8° F. The animal was euthanized due to lack of response to treatment.
Gross Pathology: The nasal mucosa was thickened, red to brown and covered by fibrin. A single cerebrocortical infarct was observed on the external surface of the brain, with multiple additional 1-3 cm red to rust colored soft lesions found after incision. Larger pale fleshy lesions were observed in kidney and testes.
Laboratory Results: Cerebrospinal fluid was obtained from the foramen magnum. It was cloudy, but became clear following centrifugation.
Protein: 589 mg/dl, Pandy 4+
RBC 29,947/ml
WBC 130/ml (25% PMN, 18% lymphs, 56% monocyte/macrophages; no
organisms seen).
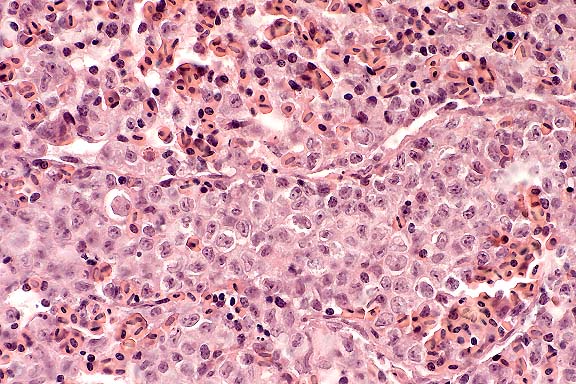
Contributor's Diagnosis and Comments: Brain: Multifocal granulomatous meningitis, with severe central necrosis and amebic cysts and trophozoites.
Amebic encephalitis is an uncommon condition of human beings and domestic animals, which results from infection by Acanthamoeba and related genera. Amebic encephalitis has been reported recently in an immunosuppressed dog and a sheep. Lesions following infection with Acanthamoeba are predominantly within the central nervous system parenchyma, and are multifocal, differing from the fulminant meningitis produced by Naegleria fowleri, a pathogen of human and nonhuman primates.
The lesions in this animal had a multifocal distribution suggestive of hematogenous dissemination, and brain lesions were mistaken for infarcts at postmortem examination. The presence of amebic lesions in kidney and testicle further suggests vascular spread. This particular patient had amebic infection of the nasal mucosa, which may have served as a source of infection for other sites. A nasal, pulmonary or skin lesion is commonly believed to be the primary source of infection in humans. Although the ram had been recently shorn, skin lesions were not observed.
Differentiation between Acanthamoeba species and related organisms is difficult in histologic specimens. Although PAS and Calcoflour white are useful in locating cysts, staining of trophs by Giemsa and mucicarmine can help differentiate them from macrophages. Immunoflourescent staining is helpful in speciation, but has not yet been done on this case. Acanthamoeba can also occasionally be observed in CSF by their motility, although it has been remarked that they are relatively less vigorous in their movements than Naegleria.
Conference Note: Infection with Balamuthia mandrillaris should be included in the differential diagnosis. This recently described free-living amoeba causes fatal meningoencephalitis in humans and old world primates.12 It has also been reported in a sheep as a cause of meningoencephalitis4, and is now considered an important emerging disease.12
Acanthamoeba and Balamuthia are morphologically similar in tissue sections at the light microscopic level; however, the presence of multiple nucleoli within trophozoite nucleosomes is a distinguishing characteristic of B. mandrillaris.12 Definitive diagnosis requires immunofluorescence studies, electron microscopy, or in vitro culture procedures. Naegleria fowleri does not form cysts in tissue sections; therefore, infection with that organism can be ruled out.
Contributor: Department of Veterinary Pathology, University of Missouri, Veterinary Medical Diagnostic Lab, P.O. Box 6023, Columbia, MO 65205
International Veterinary Pathology Slide Bank:
Laser disc frame #22131, 22132.
Terrell W. Blanchard
Major, VC, USA
Registry of Veterinary Pathology*
Department of Veterinary Pathology
Armed Forces Institute of Pathology
(202)782-2615; DSN: 662-2615
Internet: blanchard@afip.osd.mil
* The American Veterinary Medical Association and the American College of Veterinary Pathologists are co-sponsors of the Registry of Veterinary Pathology. The C.L. Davis Foundation also provides substantial support for the Registry.