Signalment: Adult, male, white faced, ovine.
History: In the late summer and fall of 1996, an extensive outbreak of disease characterized primarily by mucoid (sometimes bloody) nasal discharge, crusty muzzles, elevated temperature, oral hemorrhages and ulcers, and lameness/stiffness was seen in sheep in New Mexico. Some animals developed severe dyspnea and were treated with antibiotics for pneumonia. Blood samples were obtained from multiple animals and complete necropsies were performed on five.
Gross Pathology: The primary gross necropsy findings were well-defined, dry, pale tan areas in the papillary muscles of the heart (2 of 5) and erosion/shallow ulceration of the nares/lips/tongue (2 of 5). The lungs of the one animal which died naturally were heavy and wet on cut surface.
Laboratory Results: Bacterial culture of the lungs of two sheep revealed E. coli and alpha hemolytic Streptococcus in one, and Pasteurella sp. and Staphylococcus (coagulase negative) in the other. Joint fluid samples from one animal were culture negative for Mycoplasma and Chlamydia. Low antibody titers to Chlamydia were obtained in sera from six sheep.
EDTA blood samples from 7 of 8 sheep were positive for bluetongue (BT) viral RNA by polymerase chain reaction. Paired serum samples from 10 sheep were tested for virus neutralizing antibody titers to five strains of BT virus (10, 11, 13, 17, and 2). Six of the ten had antibody titers of ³10 to bluetongue virus strain 11. Four of the six sheep with antibody titers showed an increase in titer in the convalescent sample.
The clinical signs, gross necropsy findings, and histologic findings were considered to be indicative of bluetongue disease. Testing of whole blood samples for viral RNA and testing of sera for virus neutralizing antibody titers were necessary for a definitive diagnosis.
Additional necropsy findings in the five sheep necropsied were bronchopneumonia (2 sheep), pulmonary edema (1 sheep), and orchitis/epididymitis (2 sheep).
Conference Note: There is marked variability in the slides distributed to contributors. Demodex sp. mites, Sarcocystis sp. cysts, and a granulomatous reaction to plant material were not present in all slides. Epidermal erosions were variable.
Bluetongue (BT) is a noncontagious orbiviral (family Reoviridae)
disease of sheep, goats, and cattle. The virus is transmitted
by various species of Culicoides sp. midges (biting gnats). BT
is endemic in many areas of the world in tropical and temperate
regions. Epizootic hemorrhagic disease of deer (EHD), and Ibaraki
disease in cattle in Japan, are other orbiviral diseases similar
to BT.
Sheep are most susceptible to BT, and in that species there is
considerable variability in disease expression. Infected goats
rarely show clinical signs, and in cattle infection is almost
never associated with disease. Infected cattle serve as a reservoir,
and BT virus is likely maintained in nature by an insect-cattle
cycle, only "spilling over" into sheep and goats when
the vector population is very high.1
The pathogeneses of BT, EHD, and Ibaraki disease are similar. Following injection of the virus by the vector, primary viral replication occurs in local lymph nodes. Virus is then carried in efferent lymph to the circulation, where is it disseminated to a variety of lymphoid organs and the lungs, in which a secondary cell-associated viremia occurs. In sheep, BT virus replicates in endothelial cells in a variety of tissues. In cattle, the cellular tropism of the virus has not been completely characterized. In both sheep and cattle, virus can coexist in blood with virus-neutralizing antibodies for several weeks.1
Clinical signs of acute fulminant disease in sheep include fever, leukopenia, hyperemia of the oronasal mucosa, salivation, and nasal discharge. There may be hyperemia and edema of lips, eyelids and conjunctiva, ears, and intermandibular area. Focal hemorrhage, congestion, or cyanosis of the tongue are often seen. Erosions and ulcerations of the oral mucosa follow, and the skin of the coronary band, bulbs, and interdigital areas may be hyperemic.
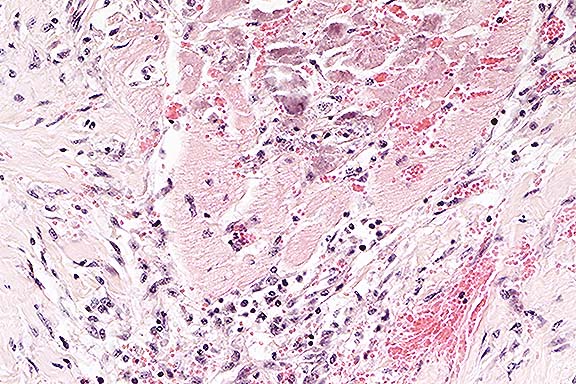
The most consistent lesion of BT is focal hemorrhage in the tunica media at the base of the pulmonary artery.5 Hemorrhage and/or edema can also be seen in the pharynx, larynx, lungs, forestomachs, abomasum, kidneys, urinary bladder, gallbladder, urethra, vulva, or prepuce. Microscopic findings are characterized by microthrombi and infarction, along with neutrophilic infiltration (early lesions) or mononuclear reaction in uncomplicated chronic lesions. There is myocardial necrosis, most prominent in the papillary muscle of the left ventricle.5
The differential diagnosis of BT in sheep should include foot-and-mouth disease, peste des petits ruminants, contagious ecthyma (Orf), and photosensitization.
International Veterinary Pathology Slide Bank:
Laser disc frame #400, 422-425, 3210.
Signalment: 4-month-old, male, Jersey, bovine.
History: Chronic diarrhea, emaciation, poor treatment response.
Gross Pathology: Enlarged mesenteric lymph nodes.
Laboratory Results: Yersinia pseudotuberculosis was isolated
from the small intestine and mesenteric lymph node. Fluorescent
antibody examinations were negative on intestinal segments for
rotavirus, coronavirus, and bovine virus diarrhea virus. Electron
microscopy examinations were negative on feces for viral particles.
Fecal flotation examinations were negative for parasite eggs,
and microscopic examination of intestines was negative for cryptosporidia.
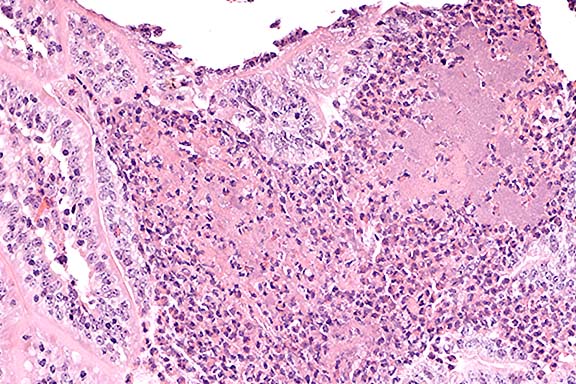
Contributor's Diagnosis and Comments: Multifocal subacute purulent enteritis with associated microcolonies of coccobacilli.
Conference Note: Yersinia pseudotuberculosis (YP) is
a gram-negative coccobacillus which causes disease in a wide range
of animal species, including birds, rodents, carnivores, cattle,
sheep, goats, captive exotic ungulates, nonhuman primates and
man.3 In man and nonhuman primates, YP causes a necrotizing, ulcerative
enteritis, sometimes with mesenteric lymphadenitis.3,5 The most
frequently seen form of disease in birds, rodents, and carnivores
is a septicemia leading to localization of the organism in liver
and spleen, with extensive caseating abscesses.3 Enterocolitis,
and rarely abortion, have been reported in cattle, sheep, and
goats. Yersiniosis in domestic animals is most significant in
Australia and New Zealand, where it is a reported cause of disease
in sheep, cattle, goats, deer and pigs.4
Yersinia pseudotuberculosis is transmitted by the fecal-oral route.
The organism contains several virulence factors, including an
invasin gene, an attachment invasion locus (ail) gene, a large
plasmid which encodes 2 outer membrane proteins that inhibit phagocytosis
and bacterial killing by host cells, and often a heat-stable enterotoxin.4
Another Yersinia species, Y. enterocolitica, causes similar disease, and the lesions caused by the two organisms cannot be differentiated reliably either grossly or microscopically. Culture is required for definitive diagnosis.
In all affected animal species, lesions in subacute to chronic yersiniosis may be mild, and are usually limited to watery intestinal content, with congestion, edema, small focal hemorrhages, or mild erosion and ulceration of the intestinal mucosa. In the colon, raised nodules with depressed centers may be seen, and mesenteric lymph nodes are often enlarged, congested, and edematous. Multifocal hepatic necrosis is sometimes a feature. In fulminant infections, there is a fibrinous or fibrinohemorrhagic enterocolitis, with mucosal colonization by large masses of coccobacilli and a marked influx of neutrophils.
International Veterinary Pathology Slide Bank:
Laser disc frame #2837, 18263, 19454, 19494, 23524, 23525.
Signalment: 1-day-old Paint filly.
History: This almost entirely white paint filly was one of a set of twins. The other twin was also almost entirely white and had been stillborn. Both the sire and dam of these fillies were overo paints. The filly had exhibited signs of abdominal pain since birth and had not passed her meconium. She was unable to rise due to a hyperflexed contracted right stifle joint. She was euthanized due to the poor prognosis.
Gross Pathology: The cecum and large colons of this filly were diffusely impacted with firm, dry, dark green, waxy meconium. The ventral colons were segmentally dilated with narrowing between dilated segments to a luminal diameter of 1-2 cm. The left dorsal colon was diffusely narrowed to a luminal diameter of 1-1.5 cm. The small colon was diffusely narrowed and constricted to a luminal diameter of less than 1 cm. It contained scant quantities of dark green, firm, waxy, meconium. The lumen of all segments of bowel was patent throughout.
The small intestine was diffusely fluid dilated and of expected luminal diameter for this age and size of foal. Jejunal contents were liquid and red-tinged. Ileal contents were thick, waxy, yellow meconium.
The right stifle joint was subluxated, with lateral displacement of the patella. The tendon attaching the patella to the quadriceps muscle was severed, folded over and partially adhered to the caudal surface of the patella. The distal end of the femur was displaced cranially in relation to the proximal tibia.
The ductus arteriosis of this filly was still patent at the time of necropsy (may be normal) but no other cardiovascular or craniofacial abnormalities were found. The stillborn twin to this filly was not available for examination.
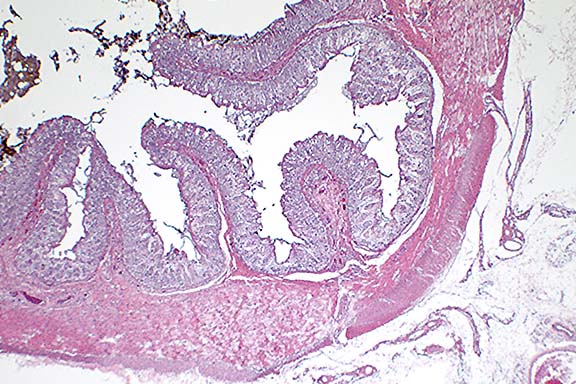
Contributor's Diagnosis and Comments: Large and small colon: diffuse colonic hypoplasia and aganglionosis with meconium impaction. (Lethal white overo trait).
Submitted tissues include longitudinal sections of portions of the large colons and a transverse section of the small colon. Subgross examination of sections of small colon reveal the extremely small diameter of this filly's colon. The small size may be due to hypoplasia. Within the muscularis, myenteric ganglia are severely reduced in number although occasional nerve fibers can be identified.
The lethal white overo foal results from the breeding of an
overo Paint stallion to an overo Paint mare. (There are two described
color patterns in paint horses; overo and tobiano. In the experience
of the contributor, tobianos are more common and have relatively
smooth edges to the margins between colored and white patches
of hair. Overos are the much less common "medicine hat"
paints with irregular, uneven edges to their coat color patches.)
The relationship between the white coat color and the lack of
myenteric plexi in the colons is proposed to be due to improper
development and migration of neural crest cells during fetal development.
Both melanocytes and the myenteric plexus are derived from the
neural crest.
This condition is similar to Hirschsprung's disease in human children,
seen in 1 in 5000 live births, and can be familial or sporadic.
In these children often only a segment of the colon or the distal
rectum is involved and leads to congenital megacolon.
Familial Hirschsprung's disease has been associated with one or more mutations in three separate genes: 1) the RET proto-oncogene, 2) the endothelin-3 (EDN-3) gene, and 3) the endothelin-B receptor (EDNR-B) gene. Mutation in RET leads to long segment Hirschsprung's disease, and mutations in EDN-3 or EDNR-B are associated with short segment Hirschsprung's disease.
The first type is an inactivating mutation (leading to loss of function) of the RET proto-oncogene. This proto-oncogene encodes a receptor tyrosine kinase that is expressed in derivatives of neural-crest cells. Activating mutations in RET (leading to enhancement of function) are associated with familial multiple endocrine neoplasia (MEN) type 2, and familial medullary thyroid carcinoma. Patients with MEN-2 frequently develop medullary thyroid carcinoma, with or without pheochromocytoma, and parathyroid hyperplasia or adenoma. (Variation is believed to be due to incomplete penetrance of the mutation). MEN-1 (triad of parathyroid, pancreatic islet cell, and anterior pituitary tumors with or without carcinoid, adrenal cortical, and lipoid tumors) is believed to be due to mutation in another gene.
Endothelin-3 knockout mice have congenital megacolon due to colonic aganglionosis and coat color spotting due to regional lack of epidermal melanocytes. Endothelin-B receptor knockout mice have the same phenotype. Mutation of this receptor gene has also been shown to be responsible for familial Hirschsprung's disease in Mennonite families. Affected humans also occasionally exhibit abnormalities in skin pigmentation. (Mutations in endothelin-1 or endothelin-A receptor results in cardiovascular or craniofacial abnormalities.)
Conference Note: Conference participants viewed a section of colon from an age-matched foal, provided by the moderator, which highlighted the remarkable hypoplasia which was especially notable in the tunica muscularis.
Three distinct isopeptides of endothelin (ET) have been identified, and are designated ET-1, ET-2, and ET-3. ET-1 is the most potent vasoconstrictor and pressor substance currently recognized.4 It is synthesized primarily by vascular endothelial cells, where along with other peptides such as thromboxane A2 it provides a signaling language between cells involved in hemostasis. Studies in mice have shown that the ET-1/ETA receptor system is essential for the development of the neural crest-derived first branchial arch.4 The ET-3/ETB receptor system, on the other hand, is essential for the normal development of two other neural crest derivatives, enteric neurons and epidermal melanocytes.4
Contributor: Searle Pharmaceuticals, 4901 Searle Parkway, Skokie, IL 60077
International Veterinary Pathology Slide Bank:
Laser disc frame #3949
Signalment: 40-hour-old, female, Standardbred horse.
History: The foal presented to the Atlantic Veterinary College with poor peripheral perfusion, severe, depression, and hypothermia. A diagnosis of septic shock was made and the foal was treated with dextrose, plasma, intravenous fluids and antibiotics. The foal died two hours after admission.
Gross Pathology: The animal was in fair body condition. Large quantities of frothy fluid were present within airways. The thoracic cavity contained approximately 200 mls of yellow, clear fluid with occasional fibrin strands. Similar fluid (500 ml) was present within the abdominal cavity. Large segments of colon were distended and congested. The lumen contained blood clots admixed with meconium. The mucosa was markedly hemorrhagic. The synovial fluid of all examined joints was turbid with flakes of fibrin.
Laboratory Results:
Bacterial isolations:
-Blood cultures - high numbers of Escherichia coli and Enterobacter
sp.
-Lung, joint fluid, liver and kidney - Escherichia coli - small
numbers
-Joint fluid:Actinobacillus equuli - high numbers
-Liver, kidney - Enterobacter sp - small numbers
-Large intestinal swab - Escherichia coli - high numbers
Enterobacter sp - high numbers
Proteus - few colonies
-Significant clinical pathological findings:
WBC: 1.5 X 109/L (normal 5.5-12.5 X 109/L)
-Blood gas analysis:
patient blood, venous Normal expected venous blood in 1-3 day
foal1
pH - 7.213 (7.38 ± 0.01)
pCO2 - 62.3 mmHg (52 ± 2)
pO2 - 30.7 mmHg (43 ± 2)
HCO3 -25.7 meq/L (29 ± 2)
1From: Koterba AM, House JK: Respiratory distress. In: Large Animal Internal Medicine, Smith BP (ed.), 2nd ed., Mosby, St. Louis, 1996, pp. 363-375.
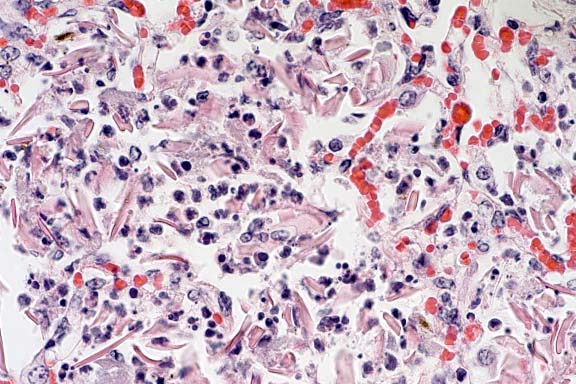
Contributor's Diagnosis and Comments: Lung: Alveolitis, acute, moderate, multifocal, suppurative with intralesional keratin and meconium.
Meconium aspiration syndrome (MAS) is an important clinicopathologic condition of neonates characterized by hypoxemia, acidosis and "patchy" atelectasis. Aspiration of amniotic fluid, with or without meconium, occurs before, during parturition, or when the umbilical cord is severed (meconium in hypopharynx). The amniotic fluid serves as a vehicle to carry fetal epidermal cells, keratin and meconium into the lungs. These materials cause a foreign body reaction and chemical alveolitis. Multinucleated giant cells are sometimes seen in the lungs of animals that have aspirated several days before. Although passage of small amounts of amniotic fluid may have little clinical significance, large amounts, as observed in this foal, cause respiratory distress, atelectasis (displacement of surfactant), inflammation, and inefficient pulmonary defense mechanisms. The long-term effect of MAS in domestic animals that survive is not known. The term alveolitis was preferred to bronchopneumonia as lesions are not grossly visible (other than focal atelectasis) and the inflammatory response is centered in the alveolar region.
Conference Note: This case was studied in consultation with the Department of Prenatal, Perinatal, and Placental Pathology of the AFIP. The peripheral acinar distribution of the inflammation is unusual for aspiration. Gram stains performed at the AFIP did not demonstrate bacteria, and a Hall's bile stain did not demonstrate meconium. Thus, the cause of the pneumonia is uncertain.
A prospective study of meconium aspiration in human infants found that 8.8% of babies are born with meconium staining of the amniotic fluid and of that group, 56% had meconium present in the trachea. Twenty percent of those with meconium staining had pulmonary disease requiring medical intervention.3 In animals, the clinicopathological significance and pathogenesis of meconium aspiration has not been well characterized. A retrospective study of 52 calves that died within the first 2 weeks of life due to a variety of causes showed that 42.5% had evidence of meconium, squamous cells, or keratin in the lung.4 The authors concluded that the clinical significance of meconium aspiration syndrome depends not on the primary lung lesions, which are seldom severe, but rather on the secondary pathophysiologic effects, such as severe acidosis and cardiopulmonary abnormalities.4
International Veterinary Pathology Slide Bank:
Laser disc frame #22199, 22200
Terrell W. Blanchard
Major, VC, USA
Registry of Veterinary Pathology*
Department of Veterinary Pathology
Armed Forces Institute of Pathology
(202)782-2615; DSN: 662-2615
Internet: blanchard@email.afip.osd.mil
* The American Veterinary Medical Association and the American
College of Veterinary Pathologists are co-sponsors of the Registry
of Veterinary Pathology. The C.L. Davis Foundation also provides
substantial support