Signalment: 23-year-old, female, Rhesus monkey (Macaca mulatta)
History: This monkey was observed to be anorexic on 23 July 97. It was anesthetized with ketamine/acepromazine and examined. Palpation of the abdomen revealed multiple discrete nodules about three to five centimeters in diameter throughout the abdomen but concentrated in the caudal region of the cavity. Radiographs of the abdomen confirmed numerous soft tissue masses in the caudal abdomen. The monkey was found dead in its cage the morning of 24 July 1997. This animal was on a dengue virus protocol and had received dengue virus vaccine in May and June of 1997. The monkey was herpes B positive, and SIV and SRV negative.
Gross Pathology: The monkey was well muscled with adequate amounts of subcutaneous and abdominal fat. The abdominal cavity was distended and contained numerous 2-5 cm dark red to tan, multilobular masses that were adhered to the mesentery, uterus (obscuring the right ovary), urinary bladder, intestines, and diaphragm. There was 140 ml of a serosanguinous fluid in the peritoneal cavity. The kidneys were bilaterally soft; the right kidney contained a cyst filled with clear fluid at its cranial pole.
Laboratory Results: Urinalysis performed postmortem: Specific gravity - 1.035; 4+ occult blood; moderate ketones; 4+ protein; pH 5.5; negative for urobilinogen, bile, and glucose; sediment exam: 2-4 erythrocytes/high power field, numerous squamous epithelial cells, numerous renal epithelial cells, and 2+ leukocytes.
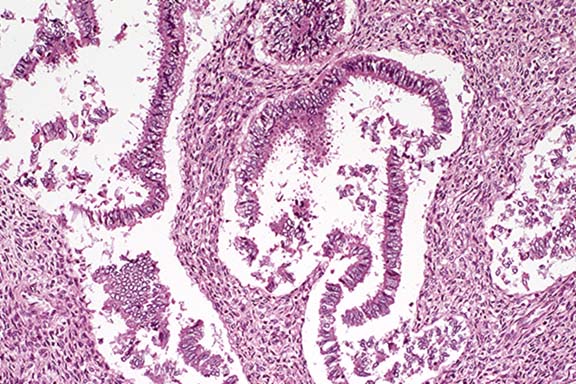
Contributor's Diagnosis and Comments: Mesentery: Endometriosis, Rhesus monkey (Macaca mulatta), non-human primate.
Endometriosis has been reported in humans, Old World monkeys and apes. Currently, there are three theories to explain the development of the lesions. The regurgitation theory involves the retrograde menstruation through the fallopian tubes which seeds endometrial tissue into the peritoneal cavity. The metaplastic theory proposes that endometrium arises directly from the coelomic epithelium, which is proposed as the origin of the endometrium itself. The last theory proposes vascular or lymphatic dissemination of endometrial tissue, which would explain the presence of endometriotic lesions in lungs or lymph nodes.
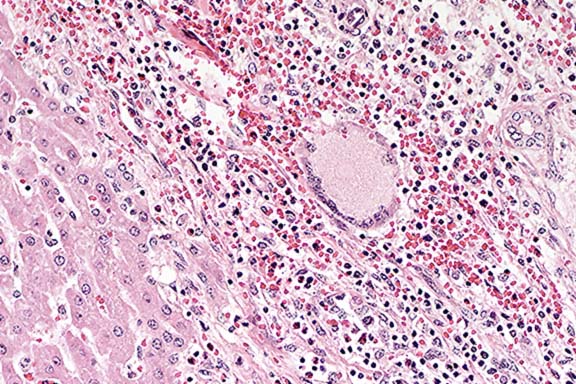
Endometriosis is the presence of viable endometrium in ectopic locations outside the uterus. Grossly, the lesions appear as soft, red, brown, or white polypoid masses adhered to the serosa of organs or mesentery and containing variable numbers of blood filled ("chocolate") cysts. Histologic features include the presence of normal appearing endometrial glands and stroma often accompanied by large amounts of hemorrhage and hemosiderin pigment. Differential diagnoses include endometrial adenocarcinoma or endometrial stromal sarcoma.
Conference Note: There was considerable variation in the slides distributed with this case. Most slides contained only a single large tissue section consisting of broad papillary fronds composed of a variably dense central stroma with embedded glandular structures and a lining of cuboidal epithelial cells. Other slides contained one or two similar but smaller tissue sections in which the specimen's papillary nature was not apparent. Additional sections obtained from the contributor after the conference demonstrated histologic features clearly consistent with endometriosis.
The nature of the stroma was debated in conference; some participants interpreted it as a fibrous stroma, since in many areas its morphology was not typical of endometrial stroma when compared to archived cases of endometriosis. In humans, a diagnosis of endometriosis requires the identification of two of the three following features: endometrial glands, stroma and hemosiderin. Hemosiderin was lacking in this specimen and the stroma was not clearly endometrial.
Although endometriosis is common in humans, its pathogenesis remains controversial and poorly understood. In addition to the 3, non-mutually exclusive, theories described by the contributor, there is evidence that immunologic factors, including peritoneal macrophages, T lymphocytes, natural killer cells, cytokines secreted by these cells, and cell adhesion molecules, are involved.5, 6
Contributor: Walter Reed Army Institute of Research, Washington, DC 20307-5100
International Veterinary Pathology Slide Bank:
Laser disc frame #7840, 19511, 21600
Signalment: 12-month-old, female, Charolais cross, bovine.
History: Eleven out of 83 yearling charolais cross calves died after acute clinical courses which lasted approximately 24 hours. Clinical signs included depression, anorexia, sunken eyes, tenesmus and slight rectal prolapse, muscle tremors, incoordination of gait, aggression, recumbency and death. The calves were being fed a ration consisting of 30% commercial ration and 70% soybean crop leftovers. These leftovers were contaminated with 5% to 25% of Xanthium cavanillesii (cocklebur) burs. The leftovers were milled, mixed to the ration and then fed to the calves. All eleven deaths occurred within a two-day period and deaths ceased after the cocklebur contaminated feed was discontinued from the animals' diet.
Gross Pathology: There was moderate to severe translucent
gelatinous edema in the abomasal ligaments, mesentery, perirenally
and in the submucosa of abomasal folds. Moderate hydropericardium
was also present. The liver was slightly swollen and had marked
accentuation of the lobular pattern. These changes were best observed
on cut surface. There were red (hemorrhagic) sunken areas surrounded
by pale, yellowish or tan colored peripheral zones. Epicardial
and endocardial petechiae and echymoses were also present. Feces
were dry and formed balls coated by mucus tinged with blood.
Laboratory Results: Serum chemistry: gGT = 42 iu/L (normal
for ox = 0-31 iu/L), FAS = 58 iu/L (normal for ox = 35-350 iu/L),
AST = 1,570 iu/L (normal for ox = 60-150 iu/L). Normal values
derived from Radostits et al, 1994.
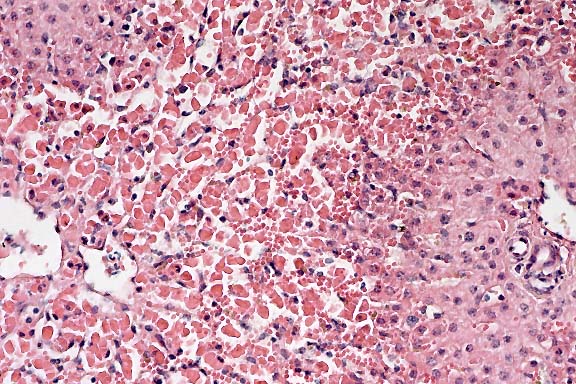
Contributor's Diagnosis and Comments: liver, hepatocellular necrosis, acute, coagulative, centrilobular, moderate to severe, with midzonal hepatocellular vacuolization.
Conference Note: Carboxyatractyloside, the toxic principle of the cocklebur plant, inhibits oxidative phosphorylation and translocation of adenine nucleotides across the mitochondrial membrane.4
Conference participants were impressed by the remarkable degree of diffuse centrilobular necrosis. Reasons for the centrilobular (periacinar) distribution of lesions caused by hepatotoxicants include 1) a relatively lower oxygenation status than that of hepatocytes in more peripheral regions of the hepatic lobule, and 2) a high concentration of cytochrome P450 mixed-function oxidase system enzymes. Other cells containing high concentrations of these enzymes include renal proximal convoluted tubular epithelium, Clara cells of the lung, and nasal epithelium.
The differential diagnosis of acute centrilobular hepatic necrosis in ruminants includes numerous plant toxins, other toxins, and, in cattle, Rift Valley fever. Notable plants include Cestrum parqui, Helichrysum blandowskianum, and Trema aspera ("poison peach"). Microcystis aeruginosa, blue-green algae growing as a bloom on lakes and ponds, is a well-documented cause of similar lesions.6
Contributor: Universidade Federal de Santa Maria, Departamento de Patologia, 97119-900, Santa Maria, RS, Brazil
International Veterinary Pathology Slide Bank:
Laser disc frame #5528, 21282, 21283.
Signalment: Adult domestic pig, breed unspecified.
History: More than 20 pigs died acutely on a farm in the endemic African swine fever control area in the northeastern part of South Africa. The pigs were accidentally being fed carcass leftovers from a warthog (Phacochoerus aethiopicus).
Gross Pathology: Cyanosis and congestion were apparent in the skin. The lymph nodes throughout the carcass were enlarged and hemorrhagic, and the abdominal cavity contained blood-tinged fluid. There was splenomegaly and the splenic parenchyma was congested and hemorrhagic. Other lesions included multiple petechiae in the renal cortices, edema, congestion and hemorrhages of the lungs and hemorrhages of the serosal surfaces.
Laboratory Results: Hemadsorbing African swine fever virus was isolated from the spleen and lymph node.
Contributor's Diagnosis and Comments: Spleen: lymphoid necrosis, depletion and loss of Schweiger-Seidel sheaths, white and red pulp, diffuse, marked with fibrinoid necrosis of small blood vessels and hemorrhage, pig, breed unspecified. Etiology: African swine fever virus.
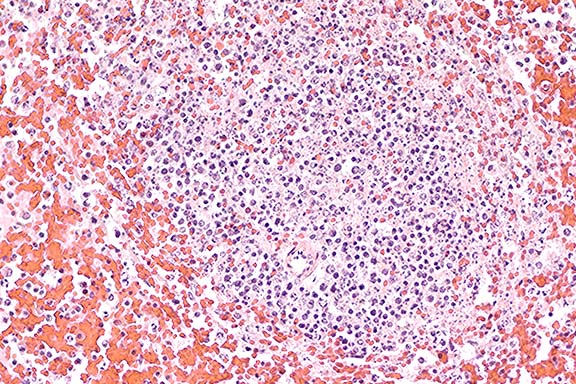
Conference Note: Vascular necrosis was present in some of the sections viewed in conference.
African swine fever (ASF) is a contagious and tick-transmitted febrile viral disease affecting the mononuclear phagocytic system. Current ASF endemic areas include sub-Saharan Africa and Sardinia. First discovered in Kenya in 1921, the disease later spread to Portugal, Spain, France, Italy, the West Indies, and more recently to Belgium (1985) and the Netherlands (1986). Large scale eradication efforts were undertaken and were successful in most of these regions.
The etiologic agent is a 200 nm enveloped DNA virus with icosahedral symmetry that replicates in the cytoplasm. Formerly classified in the Iridoviridae family, it has recently been removed from that family and is currently unclassified. It is the only known DNA arbovirus. The virus is relatively resistant to pH extremes, and can survive up to 140 days in defibrinated blood or salted and dried pork products, and 11 days in feces at room temperature.
Spread of ASF has been associated primarily with the feeding of garbage to swine. Other methods of spread include contact with blood or bloody excretions from acute or subacute cases, or by Ornithodoros sp. ticks, i.e. O. moubata in Africa and O. erraticus in Spain. Reservoirs of the virus include Ornithodoros ticks, and warthogs, which are asymptomatic carriers. Also, persistently infected pigs may serve as a source of infection for 3 to 5 months.
ASF virus enters the body orally or conjunctivally via contact with blood and blood-tinged secretions, or transdermally via tick bites. Interdigitating dendritic cells in skin and lymph nodes are the first cells infected. This leads to a failure of the immune response in acute ASF. The virus is disseminated throughout the body by attachment to erythrocytes, and causes necrosis of cells of the mononuclear phagocytic system (MPS). The spectrum of disease encountered, i.e. acute, subacute, or chronic, depends on factors such as the strain of virus, age of the pigs, and the degree of necrosis of the MPS.
Clinical signs of acute ASF include high fever for about 5 days; generalized skin erythema and cyanosis of the extremities and ears; abortion; a bleeding syndrome during the peak of the disease, including melena, which may lead to severe anemia and death; and maintenance of a good appetite even during the peak of fever.
Lesions of acute ASF include enlarged and hemorrhagic lymph nodes, especially the gastrohepatic, renal, and iliac nodes; variably enlarged friable spleen (up to 3-4 times normal size); variable hemorrhages in other organs; and pneumonia. Lungs are diffusely congested, with subpleural and interstitial hemorrhage, alveolar edema and hemorrhage, and severe interlobular edema.
Non-virus-neutralizing antibody is produced in ASF. This leads to a chronic immune-complex disease in many pigs that survive the acute disease. Chronic lesions include large hemorrhagic infarcts in the skin in areas of trauma, chronic interstitial pneumonia with caseous granulomas, chronic pericarditis, and glomerulonephritis.
The differential diagnosis includes hog cholera (classical swine fever), erysipelas, salmonellosis, warfarin toxicity, and tuberculosis (pulmonary granulomas seen in the chronic form).
International Veterinary Pathology Slide Bank:
Laser disc frame #12393, 22001-22005.
Signalment: Adult Holstein cow.
History: This milk cow was approximately 70 days pregnant with twins. It was found dead.
Gross Pathology: The referring veterinarian who performed the gross postmortem examination reported finding diffuse hemorrhages all over the heart, kidneys, omentum and intestinal mucosa.
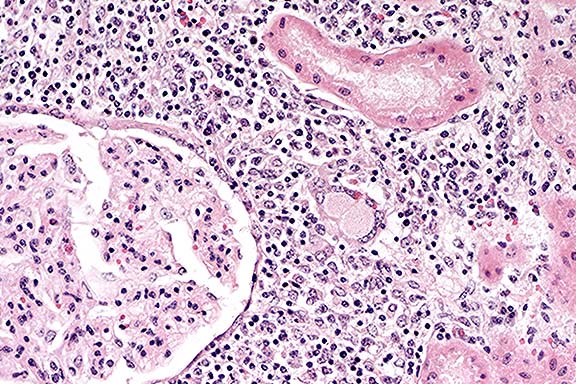
Contributor's Diagnoses and Comments: Multifocal, severe, granulomatous hepatitis and nephritis. Etiology: Hairy vetch.
The animals in this herd had been fed silage containing vetch. They may also have grazed pasture containing vetch; however, the owner was uncertain if this particular cow had been allowed to graze on pasture containing vetch. No other animals in the herd have been sick or have died recently.
Hairy vetch toxicosis has been reported in cattle and horses. The breed (Holstein) and age of cow, perivascular distribution of lesions and the type of cellular infiltrate observed in the tissues of this cow are consistent with hairy vetch toxicosis described in those reports. One difference is the apparent lack of skin lesions in this cow compared to those described in the literature. Since no skin was submitted for microscopic examination, the possibility that the cow may have had inflammatory lesions in the skin that were not readily apparent grossly can not be excluded.
Conference Note: Hairy vetch (Vicia villosa Roth) is a legume that grows throughout much of the United States and in many other temperate regions of the world. It is a widely cultivated species that is often used as pasturage, harvested as hay, ensiled, or used as a cover crop.3
Three syndromes associated with consumption of hairy vetch have been reported in cattle: (1) a syndrome of acute nervous system derangement and death after ingestion of seeds; (2) a combination of subcutaneous swellings, herpes-like eruptions in the oral mucous membranes, nasal discharge, rales, and coughing that are associated with consuming vetch pasture; and (3) a systemic granulomatous disease, also associated with vetch pasture, that is characterized clinically by dermatitis, conjunctivitis, and diarrhea.2,3 A similar granulomatous disease syndrome has also been reported in 2 horses.1,4
Vetch-associated disease is more prevalent and severe in cattle over 3 years of age. Sex predilection is inapparent. Outbreaks are most common during the season of maximal vetch growth, but sporadic cases are observed throughout the year. Previous reports have not documented illness in cattle fed vetch hay or ensiled vetch.3
The pathogenesis and specific etiologic factors of this disease are not known. The consistent lesion is a "polysystemic multifocal or confluent monocytic/lymphocytic/plasmacytic/eosinophilic/multinucleated giant cell infiltration causing enlargement and architectural disruption of the many infiltrated organs."3 One report provides circumstantial evidence that a type-IV hypersensitivity reaction is a major component of the host response.3 Alternatively, that author also suggests the possibility that vetch lectins might directly bind to T lymphocytes, activating them and stimulating production of lymphokines that mediate the cytotoxicity and granulomatous response seen in this disease.
Contributor: Department of Pathobiology, College of Veterinary Medicine, 166 Greene Hall, Auburn University, AL 36849-5519.
International Veterinary Pathology Slide Bank:
Laser disc frame #2492, 3350-3352, 4865, 20642
Terrell W. Blanchard
Major, VC, USA
Registry of Veterinary Pathology*
Department of Veterinary Pathology
Armed Forces Institute of Pathology
(202)782-2615; DSN: 662-2615
Internet: blanchard@email.afip.osd.mil
* The American Veterinary Medical Association and the American College of Veterinary Pathologists are co-sponsors of the Registry of Veterinary Pathology. The C.L. Davis Foundation also provides substantial support for the Registry.