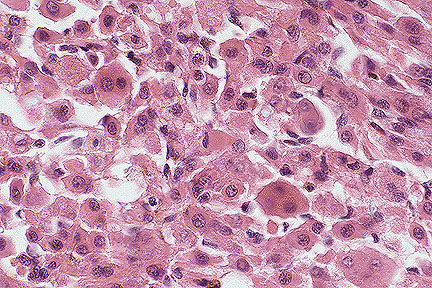
 Laryngeal rhabdomyoma in a
Cocker Spaniel. Neoplatic cells are angular, often multinucleated,
and have abundant granular eosinophilic cytoplasm. (HE, 400X,
125K)
Laryngeal rhabdomyoma in a
Cocker Spaniel. Neoplatic cells are angular, often multinucleated,
and have abundant granular eosinophilic cytoplasm. (HE, 400X,
125K)Signalment: 7 1/2-year-old castrated male Cocker Spaniel.
History: This dog presented for congested respiration and trouble barking. There was transient intermittent response to steroids, bronchodilators and antibiotics. Several months later signs had progressed to dyspnea, inspiratory stridor, vomiting and activity induced cyanosis. Thoracic radiographs revealed normal appearing lungs and a soft tissue density in the laryngeal area. Laryngeal examination showed a 2-3 cm mass displacing the left side of the larynx. The animal was euthanized and the laryngeal block submitted for histopathological evaluation.
Gross Pathology: A 5 x 3 x 2.5 cm fixed larynx is received with a 2.0 cm mass adjacent to the left vocal fold. The mass is soft, necrotic and centrally cystic and does not appear to erode or arise from laryngeal mucosa.
Laboratory Results: None submitted.
Contributor's Diagnosis and Comments: Rhabdomyoma, larynx and perilaryngeal tissue.
The neoplasm is comprised of a dense population of large individualized polyangular cells with abundant brightly eosinophilic, occasionally granular cytoplasm. Multifocally, elongate strap-shaped cells are present. Binucleate and infrequent multinucleated cells are observed. The tumor is highly vascularized with multiple foci of acute hemorrhage and hemosiderin pigment. Clear vacuolar and hyalin eosinophilic inclusions were commonly noted within nuclei. The mitotic rate is low. Individual cell degeneration is occasionally present. Phosphotungstic acid-hematoxylin stain (PTAH) revealed occasional fine cross-striations within neoplastic cells.
This tumor is consistent with canine laryngeal rhabdomyoma as described in several publications. Some of these neoplasms may have previously been mistakenly diagnosed as oncocytomas.
AFIP Diagnosis: Submucosa, perilaryngeal area: Rhabdomyoma, Cocker Spaniel, canine.
Conference Note: Rhabdomyomas are slow-growing tumors that do not metastasize and do not recur after complete surgical excision. Rhabdomyomas, oncocytomas, granular cell tumors, hibernomas, and neuroendocrine tumors are all morphologically similar in appearance, but are derived from different cell lines. These tumors are composed of large neoplastic cells with abundant granular eosinophilic cytoplasm due to the presence of either mitochondria, lysosomes, or secretory granules. Of all of these tumors, rhabdomyomas are most frequently misdiagnosed as oncocytomas.
Rhabdomyomas can be differentiated from oncocytomas and granular cell tumors by special staining procedures, immunohistochemical testing, and ultrastructural studies. The granules of rhabdomyoma cells are composed of mitochondria which stain a light blue when the cells are treated with the phosphotungstic acid-hematoxylin procedure (PTAH). In addition, some of the rhabdomyoma cells contain cross-striations which also stain blue with PTAH. Rhabdomyoma cells are usually rich in glycogen which is diastase-sensitive and can be demonstrated with the periodic acid-Schiff (PAS) procedure. Rhabdomyomas are generally immunohistochemically positive for the presence of desmin and myoglobin. Ultrastructurally they contain myofilaments and form Z bands. They lack desmosomes and are separated from each other by an external lamina.
In contrast, oncocytomas are of epithelial origin. Their cytoplasmic granularity is due to the presence of large numbers of mitochondria, a trait often shared with rhabdomyomas. Oncocytomas, however, contain no glycogen and are PAS-negative. The cytoplasmic granules of oncocytomas stain light blue with PTAH, but there are no cross-striations. They are immunohistochemically negative for desmin and myoglobin. Ultrastructurally oncocytoma cells contain large numbers of mitochondria. They lack myofilaments and are joined by desmosomes and tight junctions and are separated from the stroma by a basal lamina.
A discussion of the characteristics of granular cell tumors is included in this conference, case III.
Contributor: Department of Laboratory Animal Resources, A-115 Scaife Hall, University of Pittsburgh, Pittsburgh, PA 15261.
References:
1. Tang KN, et al: The histologic, ultrastructural and immunohistochemical
characteristics of a thyroid oncocytoma in a dog. Vet Path 31(2):269-271,
1994.
2. Liggett AD, Weiss R, and Thomas KL: Canine laryngopharyngeal
rhabdomyoma resembling an oncocytoma: Light microscopic, ultrastructural
comparative studies. Vet Path 22:526-532, 1985.
3. Meuten DJ, et al: Canine laryngeal rhabdomyoma. Vet Path 22:533-539,
1985.
4. Calderwood-Mays M: Laryngeal oncocytoma in two dogs. J Am Vet
Med Assoc 185(6):677-679, 1984.
5. Pass DA, et al: Canine laryngeal oncocytoma. Vet Path 17:672-677,
1980.
Signalment: 3-week-old Golden Retriever.
History: The puppy was presented with a 1 cm diameter subcutaneous nodule at the base of one ear. The lesion was removed at 6 weeks of age and submitted for microscopic evaluation.
Gross Pathology: An approximately 1 cm diameter cutaneous mass submitted for microscopic evaluation.
Laboratory Results: None submitted.
Contributor's Diagnosis and Comments: Rhabdomyosarcoma. Section of skin contains a densely cellular, multilobular, pleomorphic spindle-cell neoplasm. Groups of neoplastic cells are packeted by a thin encircling rim of fibrous connective tissue. Neoplastic cells are elongate with ample granular cytoplasm and indistinct cytoplasmic borders, large round to oval open-faced nuclei, and a prominent single nucleolus. Mitotic figures are frequent. A few multinucleated neoplastic cells are present; nuclei are occasionally arranged in a linear fashion. Some cells have cytoplasmic cross-striations, which were better illustrated with PTAH staining. Neoplastic cells stained positively for desmin and actin. Sarcomeric structures were visualized by transmission electron microscopy (enclosed photo).
AFIP Diagnosis: Haired skin and subcutis: Rhabdomyosarcoma, Golden Retriever, canine.
Conference Note: Rhabdomyosarcomas are malignant neoplasms that arise from striated skeletal muscle or a striated muscle progenitor cell. These tumors are highly invasive and tend to metastasize early and disseminate widely. Common sites of metastasis are lymph nodes, lung, heart, spleen, adrenal glands, kidneys, and skeletal muscle. Rhabdomyosarcomas that protrude from mucous membranes have been termed "botryoid". Botryoid rhabdomyosarcomas of the canine urinary bladder constitute two-thirds of all reported rhabdomyosarcomas in the dog.
Rhabdomyosarcomas are typically composed of pleomorphic cells arranged in long fascicles and streams. Neoplastic cells are often multinucleate, with nuclei occasionally arranged in tandem (strap cells). Cells containing larger amounts of cytoplasm often demonstrate cross-striations; visualization of these structures can be enhanced with special staining procedures, such as phosphotungstic acid-hematoxylin or silver stains. Immunohistochemically, rhabdomyosarcomas are positive for desmin and myoglobin.
Ultrastructurally, rhabdomyosarcoma cells contain actin filaments (5 nm in width) and myosin filaments (10 nm in width) that form Z-bands, I-bands, and M-bands (see electron micrograph accompanying this case). Additionally, neoplastic cells contain abundant mitochondria and glycogen, and there are indentations of the nuclear membrane.
Contributor: Roche Bioscience, 3401 Hillview Ave, Paca Alto, CA 94303.
Reference: Holland, T.J. Tumors of muscle. In Tumors in domestic animals. Ed. J.E. Moulton. University of California Press, Berkeley, CA. P 94-101.
Signalment: 10-year-old spayed female Springer Spaniel dog.
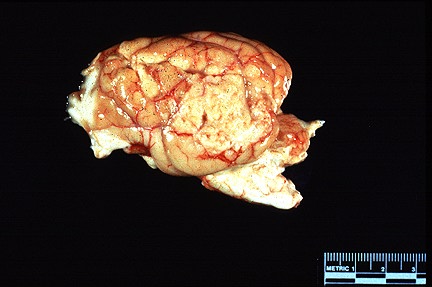 3.0 X 4.0 granular whitish-tan
neoplasm on the left temporal lobe in a Springer Spaniel. (29K)
3.0 X 4.0 granular whitish-tan
neoplasm on the left temporal lobe in a Springer Spaniel. (29K)
History: This animal had a 6 week history of neurologic signs including depression, stupor, dullness and being stuck in corners. In the three days prior to presentation, circling to the left and the inability of eat were observed. At presentation the dog circled continuously. Shortly after admission the dog began seizure-like activity and went in to respiratory arrest and was subsequently euthanized.
Gross Pathology: The animal had 3.0 x 4.0 cm white-tan, granular focus on the lateral aspect of the temporal lobe of the left cerebral hemisphere. This area and the meninges were adhered to the parietal and temporal bones. On cross-section, the mass compressed and invaded the cerebrum.
Laboratory Results: None submitted.
Contributor's Diagnosis and Comments: Cerebrum: Granular cell tumor, canine.
The meninges are focally expanded by sheets of neoplastic cells which focally compress and invade the cerebrum. The cells are variably sized (15-100 micrometers), round to polygonal with abundant granular, eosinophilic cytoplasm, numerous intracytoplasmic granules and a centrally located nucleus containing a prominent nucleolus. Mitotic figures are rare (0-1/hpf). Neoplastic cells are multifocally necrotic. Plasma cells and lymphocytes infiltrate the neoplasm in multiple foci and extend into the surrounding meninges. The intracytoplasmic granules stain strongly positive with a periodic acid-Schiff reaction.
The granular cell tumor is a rare and generally benign neoplasm that has been reported in various species including humans, dogs, horses, rats, cats and a cockatiel. In animals, granular cell tumors are most common in the dog, horse and rat. In the dog, meninges and cerebrum are atypical locations for the granular cell tumor. It is most commonly located in the oral cavity but has also been reported in the skin, heart, lymph node, meninges and cerebrum. In the horse, the neoplasm occurs only in the lung. Granular cell tumors have been reported in the brain, meninges and pituitary gland in the rat.
The origin of the granular cell tumor has been debated. Many studies have shown a neural origin but other studies have shown multiple cellular origins. This suggests that the granular cell tumor may have multiple embryologic origins. Initial immunohistochemical studies of our case (S-100 negative, glial fibrillary acidic protein negative and vimentin weakly positive) indicate a possible mesenchymal origin. However, these results are not conclusive with respect to embryologic origins.
AFIP Diagnosis: Cerebrum, meninges: Granular cell tumor, Springer Spaniel, canine.
Conference Note: Granular cell tumors have morphologic similarities to oncocytomas and rhabdomyomas, although each of these neoplasms arise from different cell-lines. Each of these neoplasms are composed of polygonal cells that have abundant cytoplasm with distinct intracytoplasmic eosinophilic granules (see case 1 of this conference), making it difficult to differentiate them histologically. Granular cell tumors are considered to be benign; however, compression of adjacent cerebral parenchyma due to expansive growth of the neoplasm is responsible for the neurologic signs noted in this case.
As the contributor notes, granular cell tumors have been described in dogs, horses, rats, a cat, a cockatiel. Granular cell tumors in each of these species contain PAS positive, diastase resistant granules. Immunohistochemical testing of granular cell tumors in these species has produced varied results. In horses, granular cell tumors were reported to be immunohistochemically positive for S-100 protein, neuron-specific enolase, and variably positive for glial fibrillary acidic protein; they were negative for actin, lysozyme, keratin, and chromogranin A. These findings are consistent with Schwann cell origin. Granular cell tumors in the dog have been reported to be positive for S-100, lysozyme and L-antitrypsin. Both granular cell tumors in the cat and the cockatiel were positive for actin; in addition, the tumor in cockatiel was positive for desmin. Most granular cell tumors in horses, dogs, cats, and rats appear to be derived from nerve sheath or meningeal cells, although other cell-lines may be involved in some cases.
Contributor: Auburn University, Department of Patholbiology, 166 Greene Hall, Al 36849-5519.
References:
1. Patnaik AK: Histologic and immunohistochemical studies of granular
cell tumors in seven dogs, three cats , one horse, and one bird.
Vet Pathol 30:176-185, 1993.
2. Engelhardt JA, Rebar AH, Honor DJ, Carlton WW: Atypical location
of granular cell tumors in two dogs. Vet Pathol 24:273-276, 1987.
3. Kelley LC, Hill JE, Hafner S, and Wortham KJ: Spontaneous equine
pulmonary granular cell tumors: Morphologic, histochemical, and
immunohistochemical characterization. Vet Pathol 32:101-106, 1995.
Signalment: Nine-year-old Quarter horse gelding.
 Patchy and crusty alopecia
in a horse. Note the depressed appearance and narrow base stance.
(41K)
Patchy and crusty alopecia
in a horse. Note the depressed appearance and narrow base stance.
(41K)
 Subcorneal pustule in a Quarter
Horse with pemphigus foliaceous. (HE, 400X, 113K)
Subcorneal pustule in a Quarter
Horse with pemphigus foliaceous. (HE, 400X, 113K)
History: Generalized crusty skin lesions of about one month's duration. Horse was depressed and reluctant to move. Euthanized after approximately one month's treatment with steroids failed to alter condition.
Gross Pathology: See history above.
Laboratory Results: None submitted.
Contributor's Diagnosis and Comments: Skin, equine, pemphigus foliaceus.
The lesions consist of multiple subcorneal pustules containing variable numbers of acanthocytes.
The roofs of many pustules have ruptured forming superficial inflammatory crusts.
The epidermis is mildly hyperplastic with light to moderate perivascular infiltration mixed inflammatory cells.
AFIP Diagnosis: Haired skin: Pustules, subcorneal, multiple, with acanthocytes, epidermal hyperplasia, serocellular crust, and mild diffuse superficial lymphoplasmacytic dermatitis, Quarter horse, equine.
Conference Note: Of the four types of pemphigus described in animals (pemphigus vulgaris, pemphigus foliaceus, pemphigus erythematosus, and pemphigus vegetans) only pemphigus foliaceus has been reported in horses. Pemphigus foliaceus is an immune-mediated skin disease that presents grossly as an exfoliative dermatitis, with crusting, seborrhea, erythema, erosions, and the formation of fragile pustules. In the horse, pemphigus foliaceus often begins on the face and neck, then gradually extends to the entire body; the genitalia and coronary bands are often affected. Over 50% of affected horses are febrile and depressed. Clinical pathology often reveals neutrophilia, hypoproteinemia, hypoalbuminemia, and anemia. Histologically, pemphigus foliaceus is characterized by subcorneal pustules and clefts that span many hair follicles. The pustules contain variable numbers of acanthocytes, neutrophils, and occasionally eosinophils. The external root sheath frequently undergoes changes similar to those of the epidermis.
Pemphigus foliaceus in humans is the result of the production of autoantibody against a cadherin adhesion molecule, desmoglein 1, which is located in desmosomes of epithelial cells. The binding of pemphigus autoantibodies stimulates secretion of a urokinase-type plasminogen activator by keratinocytes, causing a localized increase in plasmin. It is believed that the pustules form in one of two ways, either as the result of direct interruption of cell adhesion via binding of autoantibody to the adhesion molecule, and/or by the activation of plasmin, a trypsin-like endopeptidase that is capable of hydrolyzing arginine and lysine bonds, disrupting cellular adhesion.
Definitive diagnosis depends on demonstration of the autoantibody, usually IgG and IgM, in the intercellular spaces of the superficial epithelium by direct immunofluorescence. Biopsies for immunofluorescent testing should be taken from the margin of an intact pustule or the edge of a fresh lesion and quick-frozen or preserved in Michel's fixative. Immunohistochemical procedures may also be used.
Contributor: Kansas State University, Department of Diagnostic Medicine/Pathobiology, College of Veterinary Medicine, 1800 Denison Avenue, Manhattan, KS, 66506.
References:
1. Griffith, G.: Pemphigus foliaceus in a Welsh Pony. Comp. Cont.
Ed. 9:(1987):347.
2. Manning, T., and Sweeney, C.: Immune-mediated skin Diseases.
Comp. Cont. Ed. 8(1986):879.
3. Messer, W.T., and Knight, A.P.: Pemphigus foliaceus in a Horse.
JAVMA 180(1982):938.
4. Mullowney, P.C.: Dermatologic diseases of horses, Pt. V. Allergic,
immune-mediated and miscellaneous skin diseases. Comp. Cont. Ed.
7(1985):S217.
5. Cotran RS, Kumar V, Robbins SL: Pathologic basis of disease.
W.B. Saunders Co., Philadelphia, 5th edition, pp. 1201-1203, 1994.
31* The American Veterinary Medical Association and the American College of Veterinary Pathologists are co-sponsors of the Registry of Veterinary Pathology. The C.L. Davis Foundation also provides substantial support for the Registry.
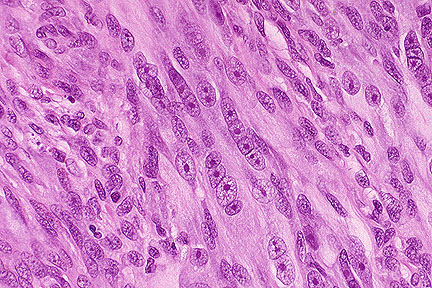 Neoplastic spindle cells with
atypical nuclei arranged in a linear fashion in a rhabdomyosarcoma
in a 3-week-old dog. (HE, 400X, 98K)
Neoplastic spindle cells with
atypical nuclei arranged in a linear fashion in a rhabdomyosarcoma
in a 3-week-old dog. (HE, 400X, 98K)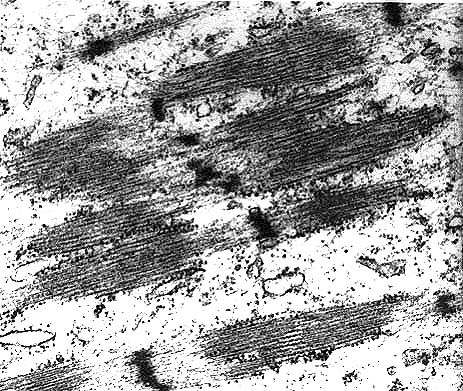 Electron micrograph of neoplastic
cells exhibiting several sarcomeres with prominent Z bands and
actin filaments.
Electron micrograph of neoplastic
cells exhibiting several sarcomeres with prominent Z bands and
actin filaments.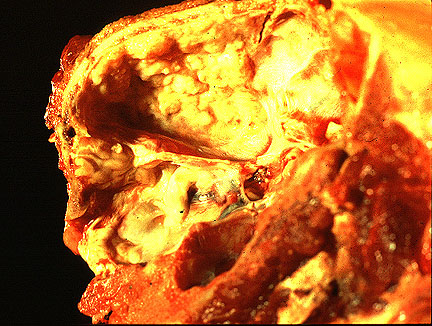 Sagittal section through the
skull of a Springer Spaniel showing a white-tan mass adherent
to the meninges. (86K)
Sagittal section through the
skull of a Springer Spaniel showing a white-tan mass adherent
to the meninges. (86K)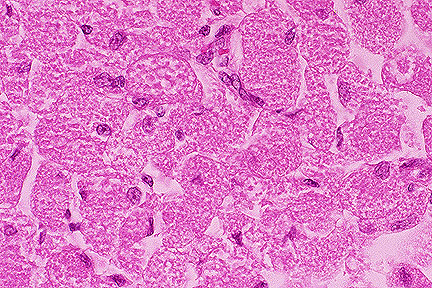 Meningeal granular cell tumor
containing polygonal cells with numerous brightly eosinophilic
cytoplasmic granules in a Springer Spaniel (HE, 400X, 156K)
Meningeal granular cell tumor
containing polygonal cells with numerous brightly eosinophilic
cytoplasmic granules in a Springer Spaniel (HE, 400X, 156K)